

Measuring mortality due to HIV-associated tuberculosis among adults in South Africa: Comparing verbal autopsy, minimally-invasive autopsy, and research data
- PMID: 28334030
- PMCID: PMC5363862
- DOI: 10.1371/journal.pone.0174097
Measuring mortality due to HIV-associated tuberculosis among adults in South Africa: Comparing verbal autopsy, minimally-invasive autopsy, and research data
Abstract
Background: The World Health Organization (WHO) aims to reduce tuberculosis (TB) deaths by 95% by 2035; tracking progress requires accurate measurement of TB mortality. International Classification of Diseases (ICD) codes do not differentiate between HIV-associated TB and HIV more generally. Verbal autopsy (VA) is used to estimate cause of death (CoD) patterns but has mostly been validated against a suboptimal gold standard for HIV and TB. This study, conducted among HIV-positive adults, aimed to estimate the accuracy of VA in ascertaining TB and HIV CoD when compared to a reference standard derived from a variety of clinical sources including, in some, minimally-invasive autopsy (MIA).
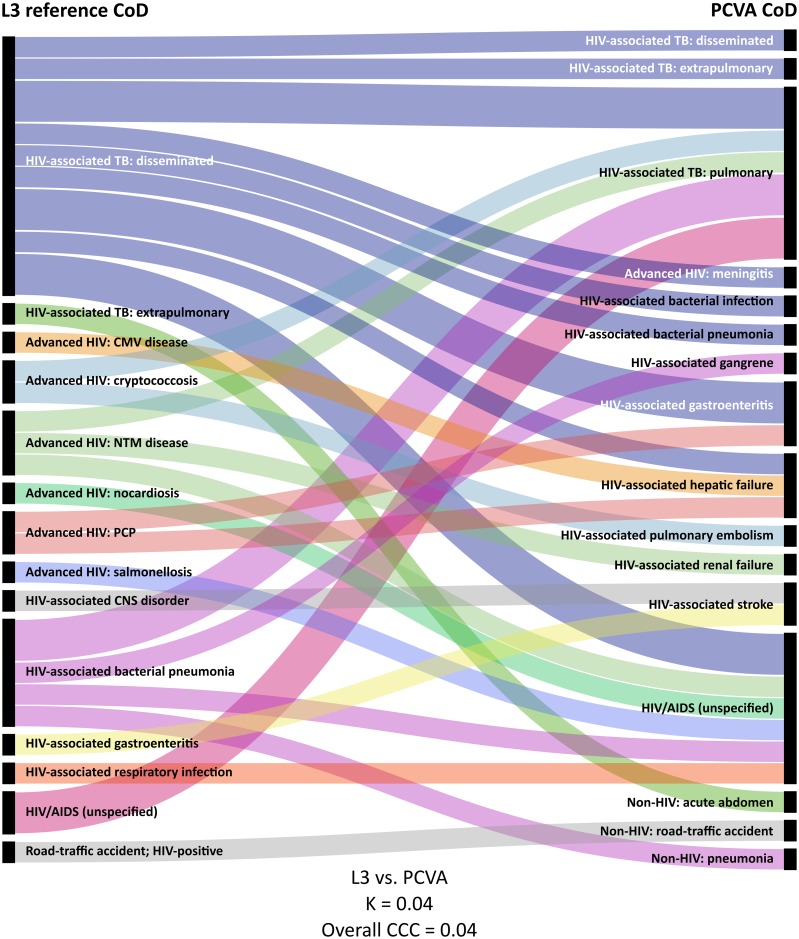
Methods and findings: Decedents were enrolled into a trial of empirical TB treatment or a cohort exploring diagnostic algorithms for TB in South Africa. The WHO 2012 instrument was used; VA CoD were assigned using physician-certified VA (PCVA), InterVA-4, and SmartVA-Analyze. Reference CoD were assigned using MIA, research, and health facility data, as available. 259 VAs were completed: 147 (57%) decedents were female; median age was 39 (interquartile range [IQR] 33-47) years and CD4 count 51 (IQR 22-102) cells/μL. Compared to reference CoD that included MIA (n = 34), VA underestimated mortality due to HIV/AIDS (94% reference, 74% PCVA, 47% InterVA-4, and 41% SmartVA-Analyze; chance-corrected concordance [CCC] 0.71, 0.42, and 0.31, respectively) and HIV-associated TB (41% reference, 32% PCVA; CCC 0.23). For individual decedents, all VA methods agreed poorly with reference CoD that did not include MIA (n = 259; overall CCC 0.14, 0.06, and 0.15 for PCVA, InterVA-4, and SmartVA-Analyze); agreement was better at population level (cause-specific mortality fraction accuracy 0.78, 0.61, and 0.57, for the three methods, respectively).
Conclusions: Current VA methods underestimate mortality due to HIV-associated TB. ICD and VA methods need modifications that allow for more specific evaluation of HIV-related deaths and direct estimation of mortality due to HIV-associated TB.
Conflict of interest statement
Figures

References
-
- Joint United Nations Programme on HIV/AIDS. AIDSinfo. 2015 [accessed 23 Feb 2017]. http://aidsinfo.unaids.org/
-
- World Health Organization. Global tuberculosis report 2015. 2015 [accessed 29 Sep 2016]. http://www.who.int/tb/publications/global_report/en/
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
