

Vestibular Aqueduct Midpoint Width and Hearing Loss in Patients With an Enlarged Vestibular Aqueduct
- PMID: 28334328
- PMCID: PMC5824227
- DOI: 10.1001/jamaoto.2016.4522
Vestibular Aqueduct Midpoint Width and Hearing Loss in Patients With an Enlarged Vestibular Aqueduct
Abstract
Importance: Elucidating the relationship between vestibular aqueduct size and hearing loss progression may inform the prognosis and counseling of patients who have an enlarged vestibular aqueduct (EVA).
Objectives: To examine the association between vestibular aqueduct size and repeated measures of hearing loss.
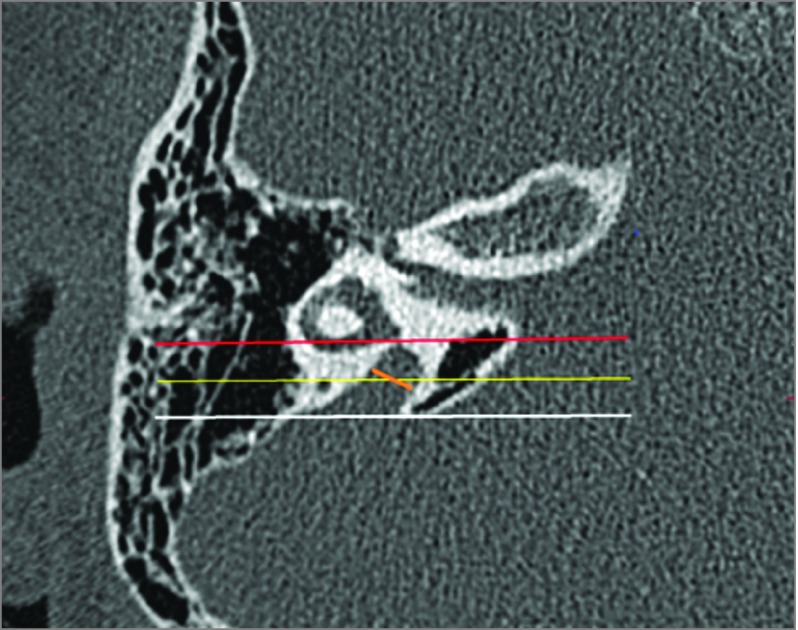
Design, setting, and participants: For this retrospective medical record review, 52 patients with a diagnosis of hearing loss and radiologic diagnosis of EVA according to the Valvassori criterion were included. All available speech reception threshold and word recognition score data was retrieved; mixed-effects models were constructed where vestibular aqueduct size, age at diagnosis of hearing loss, and time since diagnosis of hearing loss were used to predict repeated measures of hearing ability. This study was performed at an academic tertiary care center.
Exposures: Variable vestibular aqueduct size, age at first audiogram, length of time after first audiogram.
Main outcomes and measures: Speech reception threshold (dB) and word recognition score (%) during routine audiogram.
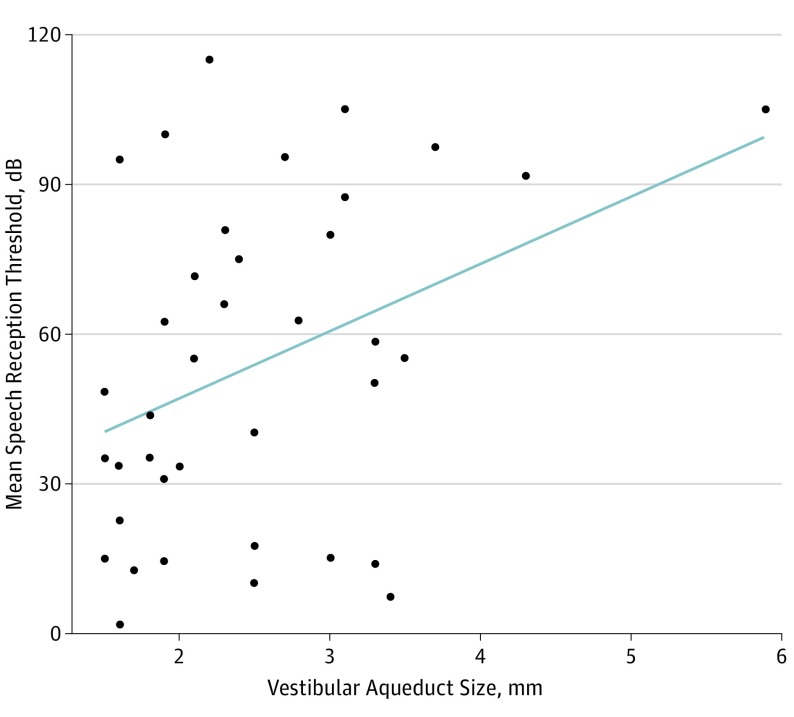
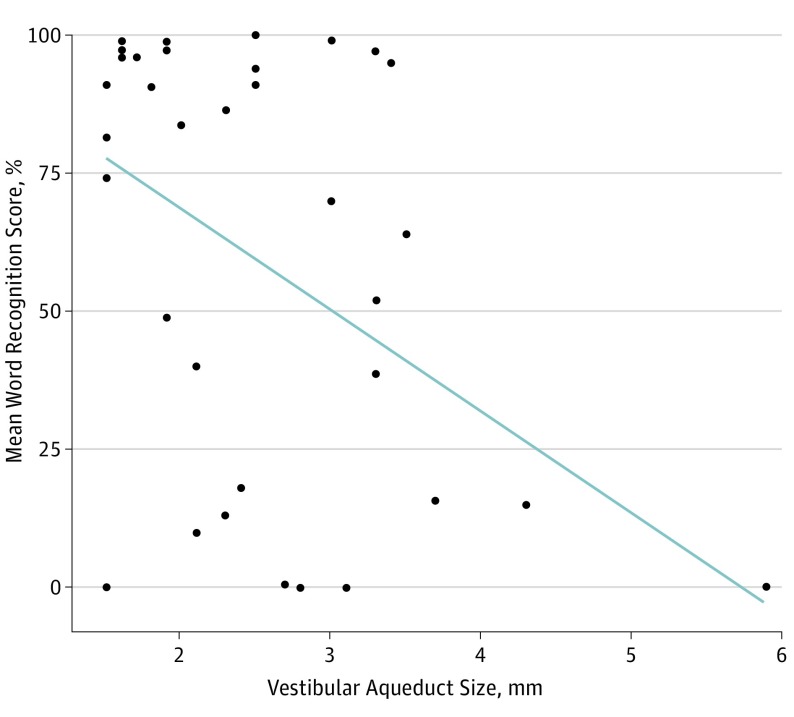
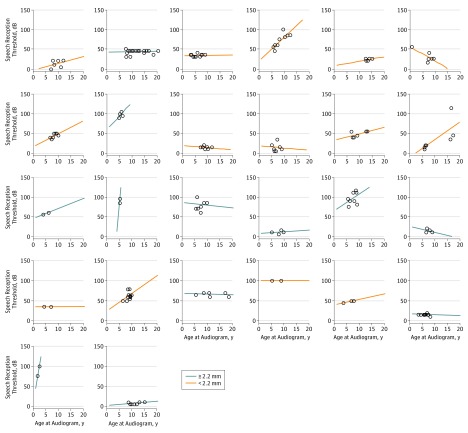
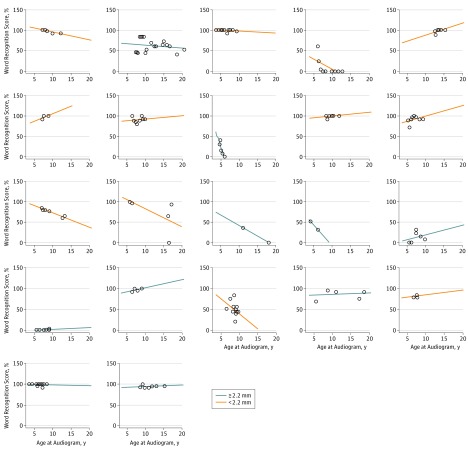
Results: Overall, 52 patients were identified (29 females [56%] and 23 males [44%]; median age at all recorded audiograms, 7.8 years) with a total of 74 ears affected by EVA. Median (range) vestibular aqueduct size was 2.15 (1.5-5.9) mm, and a median (range) of 5 (1-18) tests were available for each patient. Each millimeter increase in vestibular aqueduct size above 1.5 mm was associated with an increase of 17.5 dB in speech reception threshold (95% CI, 7.2 to 27.9 dB) and a decrease of 21% in word recognition score (95% CI, -33.3 to -8.0 dB). For each extra year after a patient's first audiogram, there was an increase of 1.5 dB in speech recognition threshold (95% CI, 0.22 to 3.0 dB) and a decrease of 1.7% in word recognition score (95% CI, -3.08 to -0.22 dB).
Conclusions and relevance: Hearing loss in patients with an EVA is likely influenced by vestibular aqueduct midpoint width. When considering hearing loss prognosis, vestibular aqueduct midpoint width may be useful for the clinician who counsels patients affected by EVA.
Conflict of interest statement
Figures
Similar articles
-
Retrospective Review of Midpoint Vestibular Aqueduct Size in the 45° Oblique (Pöschl) Plane and Correlation with Hearing Loss in Patients with Enlarged Vestibular Aqueduct.AJNR Am J Neuroradiol. 2021 Dec;42(12):2215-2221. doi: 10.3174/ajnr.A7339. Epub 2021 Nov 4. AJNR Am J Neuroradiol. 2021. PMID: 34737185 Free PMC article.
-
Hearing loss in unilateral and bilateral enlarged vestibular aqueduct syndrome.Int J Pediatr Otorhinolaryngol. 2019 Mar;118:147-151. doi: 10.1016/j.ijporl.2018.12.023. Epub 2018 Dec 19. Int J Pediatr Otorhinolaryngol. 2019. PMID: 30634102
-
Hearing loss in enlarged vestibular aqueduct and incomplete partition type II.Am J Otolaryngol. 2017 Nov-Dec;38(6):692-697. doi: 10.1016/j.amjoto.2017.06.010. Epub 2017 Jun 23. Am J Otolaryngol. 2017. PMID: 28793961
-
Hearing Loss in Enlarged Vestibular Aqueduct: A Prognostic Factor Systematic Review of the Literature.Otol Neurotol. 2021 Jan;42(1):99-107. doi: 10.1097/MAO.0000000000002843. Otol Neurotol. 2021. PMID: 33026783
-
Enlarged vestibular aqueduct: review of controversial aspects.Laryngoscope. 2011 Sep;121(9):1971-8. doi: 10.1002/lary.22083. Epub 2011 Aug 16. Laryngoscope. 2011. PMID: 22024854 Review.
Cited by
-
Is CT or MRI the optimal imaging investigation for the diagnosis of large vestibular aqueduct syndrome and large endolymphatic sac anomaly?Eur Arch Otorhinolaryngol. 2019 Mar;276(3):693-702. doi: 10.1007/s00405-019-05279-x. Epub 2019 Jan 11. Eur Arch Otorhinolaryngol. 2019. PMID: 30635710 Free PMC article.
-
Fluid-solid coupling model and biological features of large vestibular aqueduct syndrome.Front Bioeng Biotechnol. 2023 May 11;11:1106371. doi: 10.3389/fbioe.2023.1106371. eCollection 2023. Front Bioeng Biotechnol. 2023. PMID: 37251559 Free PMC article.
-
Retrospective Review of Midpoint Vestibular Aqueduct Size in the 45° Oblique (Pöschl) Plane and Correlation with Hearing Loss in Patients with Enlarged Vestibular Aqueduct.AJNR Am J Neuroradiol. 2021 Dec;42(12):2215-2221. doi: 10.3174/ajnr.A7339. Epub 2021 Nov 4. AJNR Am J Neuroradiol. 2021. PMID: 34737185 Free PMC article.
-
Exploring the missing heritability in subjects with hearing loss, enlarged vestibular aqueducts, and a single or no pathogenic SLC26A4 variant.Hum Genet. 2022 Apr;141(3-4):465-484. doi: 10.1007/s00439-021-02336-6. Epub 2021 Aug 19. Hum Genet. 2022. PMID: 34410491 Free PMC article.
-
Auditory and imaging markers of atypical enlarged vestibular aqueduct.Eur Arch Otorhinolaryngol. 2022 Feb;279(2):695-702. doi: 10.1007/s00405-021-06700-0. Epub 2021 Mar 9. Eur Arch Otorhinolaryngol. 2022. PMID: 33687508
References
-
- Berrettini S, Forli F, Bogazzi F, et al. . Large vestibular aqueduct syndrome: audiological, radiological, clinical, and genetic features. Am J Otolaryngol. 2005;26(6):363-371. - PubMed
-
- Arcand P, Desrosiers M, Dubé J, Abela A. The large vestibular aqueduct syndrome and sensorineural hearing loss in the pediatric population. J Otolaryngol. 1991;20(4):247-250. - PubMed
-
- Alemi AS, Chan DK. Progressive hearing loss and head trauma in enlarged vestibular aqueduct: a systematic review and meta-analysis. Otolaryngol Head Neck Surg. 2015;153(4):512-517. - PubMed
-
- Usami S, Abe S, Weston MD, Shinkawa H, Van Camp G, Kimberling WJ. Non-syndromic hearing loss associated with enlarged vestibular aqueduct is caused by PDS mutations. Hum Genet. 1999;104(2):188-192. - PubMed
-
- Kemperman MH, Stinckens C, Kumar S, Huygen PL, Joosten FB, Cremers CW. Progressive fluctuant hearing loss, enlarged vestibular aqueduct, and cochlear hypoplasia in branchio-oto-renal syndrome. Otol Neurotol. 2001;22(5):637-643. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
