

Capnography versus standard monitoring for emergency department procedural sedation and analgesia
- PMID: 28334427
- PMCID: PMC6353146
- DOI: 10.1002/14651858.CD010698.pub2
Capnography versus standard monitoring for emergency department procedural sedation and analgesia
Abstract
Background: Procedural sedation and analgesia (PSA) is used frequently in the emergency department (ED) to facilitate painful procedures and interventions. Capnography, a monitoring modality widely used in operating room and endoscopy suite settings, is being used more frequently in the ED setting with the goal of reducing cardiopulmonary adverse events. As opposed to settings outside the ED, there is currently no consensus on whether the addition of capnography to standard monitoring modalities reduces adverse events in the ED setting.
Objectives: To assess whether capnography in addition to standard monitoring (pulse oximetry, blood pressure and cardiac monitoring) is more effective than standard monitoring alone to prevent cardiorespiratory adverse events (e.g. oxygen desaturation, hypotension, emesis, and pulmonary aspiration) in ED patients undergoing PSA.
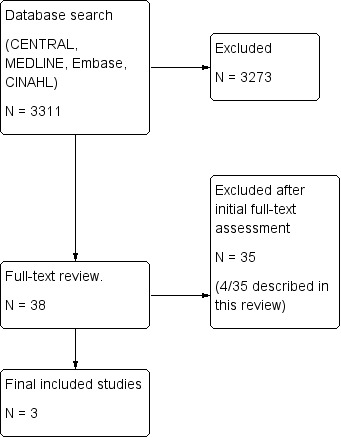
Search methods: We searched the Cochrane Central Register of Controlled Trials (2016, Issue 8), and MEDLINE, Embase, and CINAHL to 9 August 2016 for randomized controlled trials (RCTs) and quasi-randomized trials of ED patients requiring PSA with no language restrictions. We searched meta-registries (www.controlled-trials.com, www.clinicalstudyresults.org, and clinicaltrials.gov) for ongoing trials (February 2016). We contacted the primary authors of included studies as well as scientific advisors of capnography device manufacturers to identify unpublished studies (February 2016). We handsearched conference abstracts of four organizations from 2010 to 2015.
Selection criteria: We included any RCT or quasi-randomized trial comparing capnography and standard monitoring to standard monitoring alone for ED patients requiring PSA.
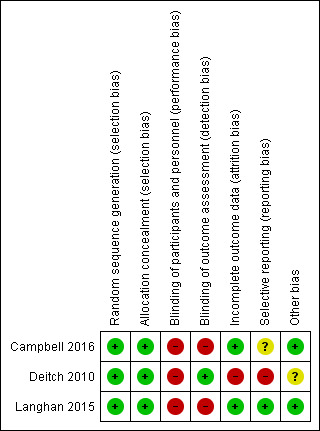
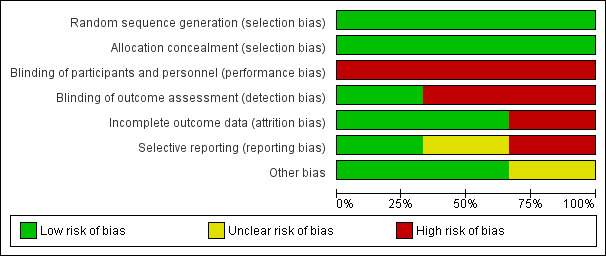
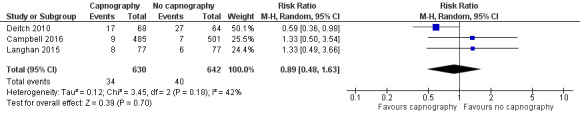
Data collection and analysis: Two authors independently performed study selection, data extraction, and assessment of methodological quality for the 'Risk of bias' tables. An independent researcher extracted data for any included studies that our authors were involved in. We contacted authors of included studies for incomplete data when applicable. We used Review Manager 5 to combine data and calculate risk ratios (RR) and 95% confidence intervals (CI) using both random-effects and fixed-effect models.
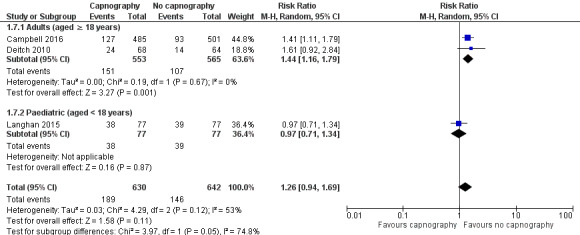
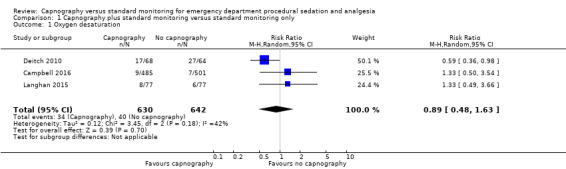
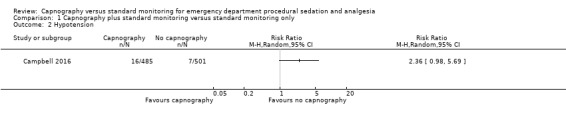
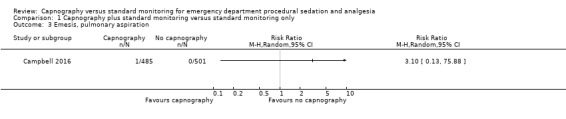
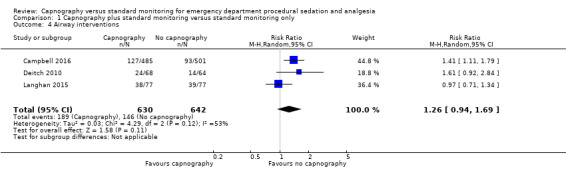
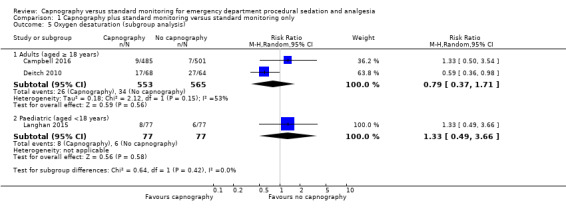
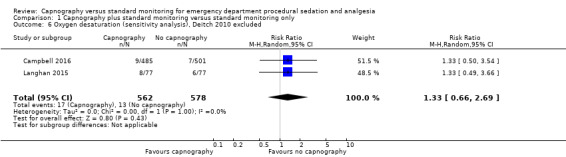
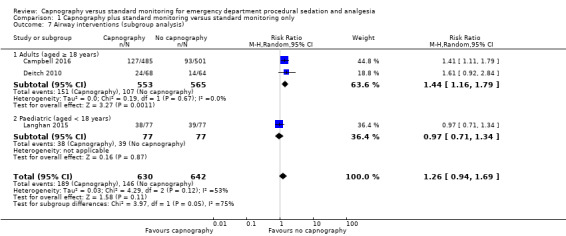
Main results: We identified three trials (κ = 1.00) involving 1272 participants. Comparing the capnography group to the standard monitoring group, there were no differences in the rates of oxygen desaturation (RR 0.89, 95% CI 0.48 to 1.63; n = 1272, 3 trials; moderate quality evidence) and hypotension (RR 2.36, 95% CI 0.98 to 5.69; n = 986, 1 trial; moderate quality evidence). There was only one episode of emesis recorded without significant difference between the groups (RR 3.10, 95% CI 0.13 to 75.88, n = 986, 1 trial; moderate quality evidence). The quality of evidence for the primary outcomes was moderate with downgrades primarily due to heterogeneity and reporting bias.There were no differences in the rate of airway interventions performed (RR 1.26, 95% CI 0.94 to 1.69; n = 1272, 3 trials; moderate quality evidence). In the subgroup analysis, we found a higher rate of airway interventions for adults in the capnography group (RR 1.44, 95% CI 1.16 to 1.79; n = 1118, 2 trials; moderate quality evidence) with a number needed to treat for an additional harmful outcome of 12. Although statistical heterogeneity was reduced, there was moderate quality of evidence due to outcome definition heterogeneity and limited reporting bias. None of the studies reported recovery time.
Authors' conclusions: There is a lack of convincing evidence that the addition of capnography to standard monitoring in ED PSA reduces the rate of clinically significant adverse events. Evidence was deemed to be of moderate quality due to population and outcome definition heterogeneity and limited reporting bias. Our review was limited by the small number of clinical trials in this setting.
Conflict of interest statement
Brian F Wall: none known.
Kirk Magee: was a listed author of one of the included studies in this review (Campbell 2016).
Samuel G Campbell: was a listed author of one of the included studies in this review (Campbell 2016).
Peter J Zed: was a listed author of one of the included studies in this review (Campbell 2016).
Figures

Comment in
-
What Is the Utility of End-Tidal Capnography for Procedural Sedation and Analgesia in the Emergency Department?Ann Emerg Med. 2017 Dec;70(6):819-821. doi: 10.1016/j.annemergmed.2017.06.035. Epub 2017 Jul 26. Ann Emerg Med. 2017. PMID: 28754357 No abstract available.
References
References to studies included in this review
Campbell 2016 {published and unpublished data}
Deitch 2010 {published data only}
-
- Deitch K, Miner J, Chudnofsky CR, Dominici P, Latta D. Does end tidal CO2 monitoring during emergency department procedural sedation and analgesia with propofol decrease the incidence of hypoxic events? A randomized, controlled trial. Annals of Emergency Medicine 2010;5(3):258‐64. [DOI: 10.1016/j.annemergmed.2009.07.030; PUBMED: 19783324] - DOI - PubMed
References to studies excluded from this review
Deitch 2007 {published data only}
-
- Deitch K, Chudnofsky CR, Dominici P. The utility of supplemental oxygen during emergency department procedural sedation and analgesia with midazolam and fentanyl: a randomized, controlled trial. Annals of Emergency Medicine 2007;49(1):1‐8. [PUBMED: 16978741] - PubMed
Deitch 2008 {published data only}
-
- Deitch K, Chudnofsky CR, Dominici P. The utility of supplemental oxygen during emergency department procedural sedation with propofol: a randomized, controlled trial. Annals of Emergency Medicine 2008;52(1):1‐8. [PUBMED: 18294729] - PubMed
Hart 1997 {published data only}
-
- Hart LS, Berns SD, Houck CS, Boenning DA. The value of end‐tidal CO2 monitoring when comparing three methods of conscious sedation for children undergoing painful procedures in the emergency department. Pediatric Emergency Care 1997;13(3):189‐93. [PUBMED: 9220504] - PubMed
Sivilotti 2010 {published data only}
-
- Sivilotti MLA, Messenger DW, Vlymen J, Dungey PE, Murray HE. A comparative evaluation of capnometry versus pulse oximetry during procedural sedation and analgesia on room air. Canadian Journal of Emergency Medicine 2010;12(5):397‐404. [PUBMED: 20880431] - PubMed
Additional references
Anderson 2007
-
- Anderson JL, Junkins E, Pribble C, Guenther E. Capnography and depth of sedation during propofol sedation in children. Annals of Emergency Medicine 2007;49:9‐13. - PubMed
Burton 2006
-
- Burton JH, Harrah JD, Germann CA, Dillon DC. Does end‐tidal carbon dioxide monitoring detect respiratory events prior to current sedation monitoring practices?. Academic Emergency Medicine 2006;13(5):500‐4. - PubMed
Burton 2012
-
- Burton F. Towards evidence based emergency medicine: best BETs from the Manchester Royal Infirmary. BET 2: should capnography be routinely used during procedural sedation in the emergency department?. Emergency Medicine Journal 2012;29:164‐6. - PubMed
Campbell 2006
-
- Campbell SG, Magee KD, Kovacs GJ, Petrie DA, Tallon JM, McKinley R, et al. Procedural sedation and analgesia in a Canadian adult tertiary care emergency department: a case series. Canadian Journal of Emergency Medicine 2006;8(2):85‐93. - PubMed
Cudny 2013
Egger 1997
EndNote X7.4 [Computer program]
-
- Thomson Reuters. EndNote X7.4. Thomson Reuters, 2015.
Godwin 2005
-
- Godwin SA, Caro DA, Wolf SJ, Jagoda AS, Charles R, Marett BE, et al. American College of Emergency Physicians. Clinical policy: procedural sedation and analgesia in the emergency department. Annals of Emergency Medicine 2005;45:177‐96. - PubMed
Godwin 2014
-
- Godwin S, Burton J, Gerardo C, Hatten B, Mace S, Silvers S, et al. Clinical Policy: Procedural Sedation and Analgesia in the Emergency Department. Annals of Emergency Medicine 2014;63:247‐58. - PubMed
Green 2010
-
- Green SM, Pershad J. Should capnographic monitoring be standard practice during emergency department procedural sedation and analgesia? Pro and con. Annals of Emergency Medicine 2010;55:265‐7. - PubMed
Guyatt 2008
Higgins 2011
-
- Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Kodali 2013
-
- Kodali BS. Capnography outside the operating rooms. Anesthesiology 2013;118:192‐201. - PubMed
Krauss 2007
-
- Krauss B, Hess DR. Capnography for procedural sedation and analgesia in the emergency department. Annals of Emergency Medicine 2007;50:172‐81. [PUBMED: 17222941 ] - PubMed
Langhan 2012
-
- Langhan ML, Mallory M, Hertzog J, Lowrie L, Cravero J. Physiologic monitoring practices during pediatric procedural sedation. A report from the Pediatric Sedation Research Consortium. Archives of Pediatrics & Adolescent Medicine 2012;166:990‐8. - PubMed
Mallory 2011
-
- Mallory MD, Baxter AL, Yanosky DJ, Cravero JP. Emergency physician administered propofol sedation: a report on 25,433 sedations from the Pediatric Sedation Research Consortium. Annals of Emergency Medicine 2011;57:462‐8. - PubMed
McCarney 2007
Miner 2002
-
- Miner JR, Heegaard W, Plummer D. End‐tidal carbon dioxide monitoring during procedural sedation. Academic Emergency Medicine 2002;9:275‐80. - PubMed
Miner 2003
-
- Miner JR, Biros M, Krieg S, Johnson C, Heegaard W, Plummer D. Randomized clinical trial of propofol versus methohexital for procedural sedation in the emergency department. Academic Emergency Medicine 2003;10:931‐7. - PubMed
Mohr 2013
-
- Mohr NM, Wessman B. Routine capnography in procedural sedation. Annals of Emergency Medicine 2013;61:697‐8. - PubMed
RevMan 2014 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Saretsky 1972
-
- Saretsky G. The OEO P.C. Experiment and the John Henry Effect. The Phi Delta Kappan 1972;53(9):579‐81.
Sealed 2012
-
- Sealed Envelope Ltd. 2012. Power calculator for binary outcome superiority trial. [Online]. www.sealedenvelope.com/power/binary‐superiority/ (last accessed 15 June 2016).
Swanson 1996
-
- Swanson E, Seaberg DC, Mathias S. The use of propofol for sedation in the emergency department. Academic Emergency Medicine 1996;3:234‐8. - PubMed
Wright 1992
-
- Wright SW. Conscious sedation in the emergency department: the value of capnography and pulse oximetry. Annals of Emergency Medicine 1992;21:551‐5. - PubMed
References to other published versions of this review
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous