

Time-dependent association of glucocorticoids with adverse outcome in community-acquired pneumonia: a 6-year prospective cohort study
- PMID: 28335807
- PMCID: PMC5364618
- DOI: 10.1186/s13054-017-1656-7
Time-dependent association of glucocorticoids with adverse outcome in community-acquired pneumonia: a 6-year prospective cohort study
Abstract
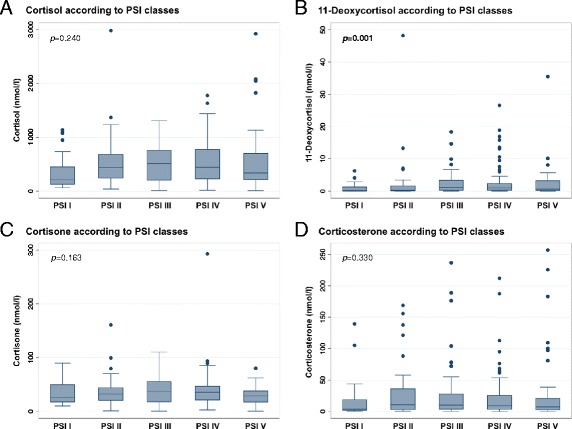
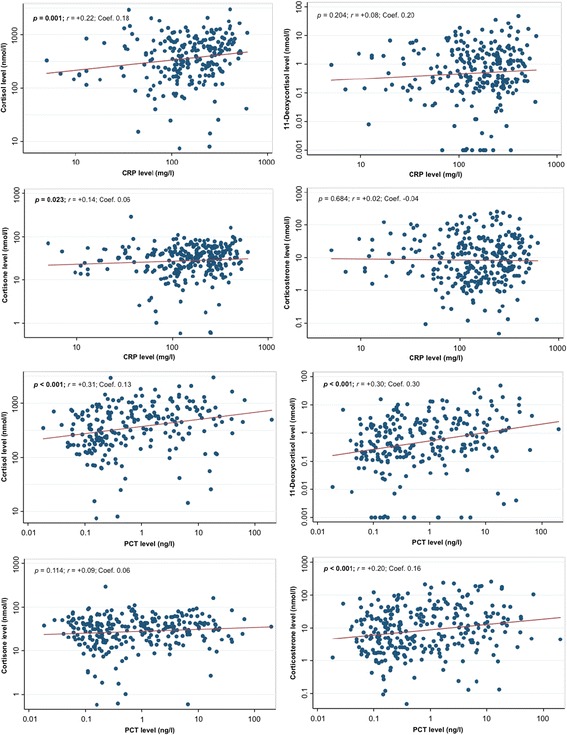
Background: The hypothalamic-pituitary-adrenal stress axis plays a crucial role in community-acquired pneumonia (CAP), with high cortisol being associated with disease severity and corticosteroid treatment resulting in earlier time to recovery. Our aim in the present study was to compare different glucocorticoid hormones, including cortisol, 11-deoxycortisol, cortisone, and corticosterone, regarding their association with short- and long-term adverse outcomes in a well-defined CAP cohort.
Methods: We prospectively followed 285 patients with CAP from a previous Swiss multicenter trial for a median of 6.1 years and measured different admission glucocorticoid serum levels by liquid chromatography coupled with tandem mass spectrometry. We used adjusted Cox regression models to investigate associations between admission hormone levels and all-cause mortality at different time points.
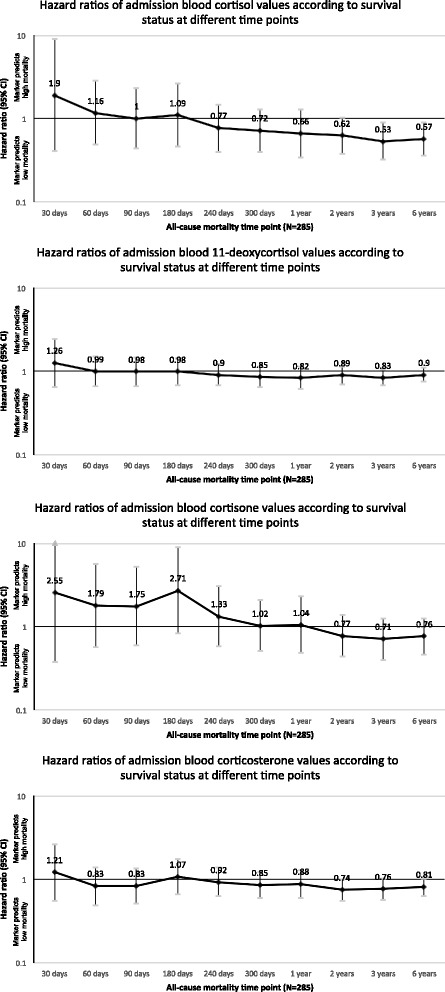
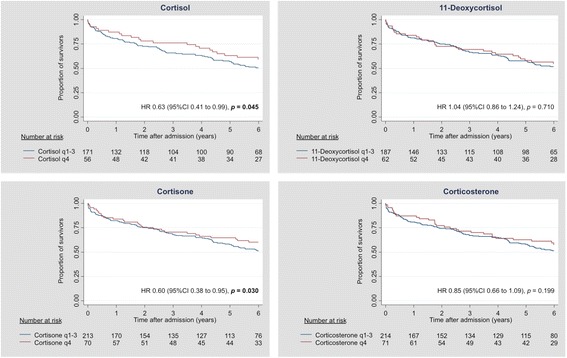
Results: Mortality was 5.3% after 30 days and increased to 47.3% after 6 years. High admission cortisol was associated with adverse outcome after 30 days (adjusted OR 3.85, 95% CI 1.10-13.49, p = 0.035). In the long term (i.e.,), however, high admission cortisol was associated with better survival (adjusted HR after 3 years 0.53, 95% CI 0.32-0.89, p = 0.017; adjusted HR after 6 years 0.57, 95% CI 0.36-0.90, p = 0.015). Compared with 11-deoxycortisol, cortisone, and corticosterone, cortisol showed the highest association with mortality.
Conclusions: Among different glucocorticoid hormones, cortisol showed the highest association with mortality in CAP. Whereas a more pronounced glucocorticoid stress response on hospital admission was associated with higher short-term adverse outcome, long-term outcome was favorable in these patients. These data should support the correct interpretation of glucocorticoid blood data.
Keywords: 11-Deoxycortisol; Community-acquired pneumonia; Corticosterone; Cortisol; Cortisone; Disease severity; Glucocorticoid hormones; Mortality/outcome prediction; Pneumonia severity index.
Figures
References
-
- Van den Berghe G, de Zegher F, Bouillon R. Clinical review 95: acute and prolonged critical illness as different neuroendocrine paradigms. J Clin Endocrinol Metab. 1998;83(6):1827–34. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
