

Network degeneration and dysfunction in presymptomatic C9ORF72 expansion carriers
- PMID: 28337409
- PMCID: PMC5349617
- DOI: 10.1016/j.nicl.2016.12.006
Network degeneration and dysfunction in presymptomatic C9ORF72 expansion carriers
Abstract
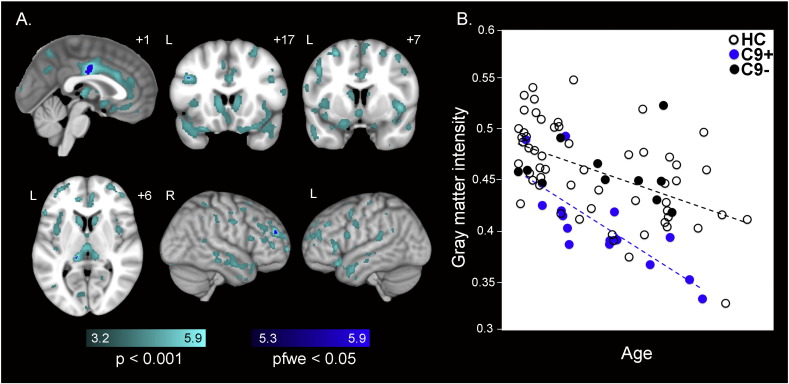
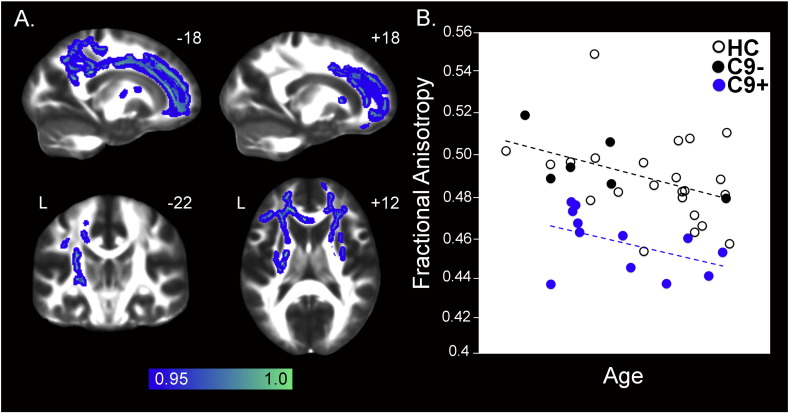
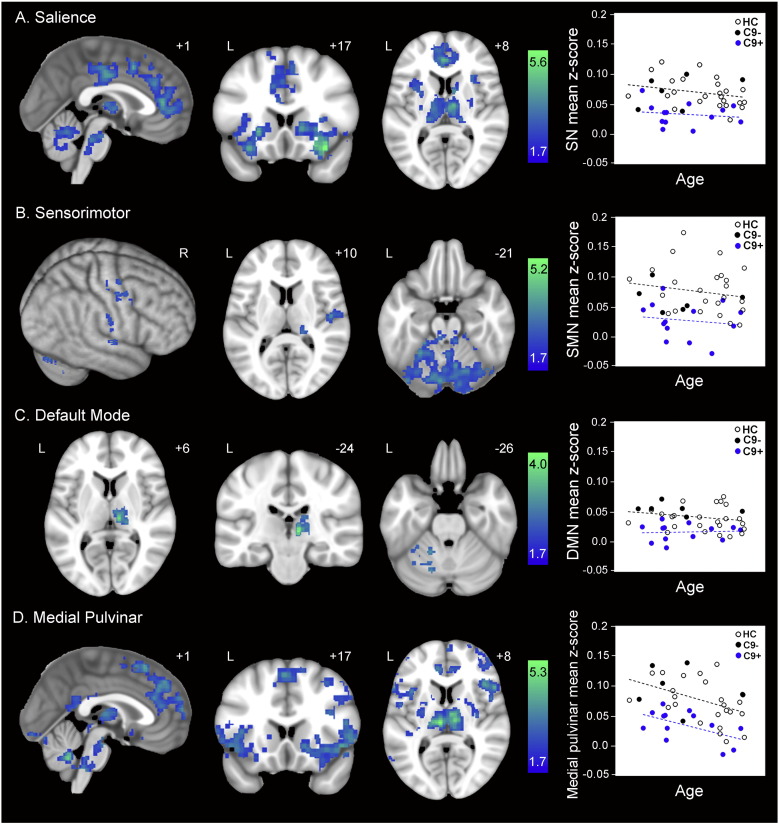
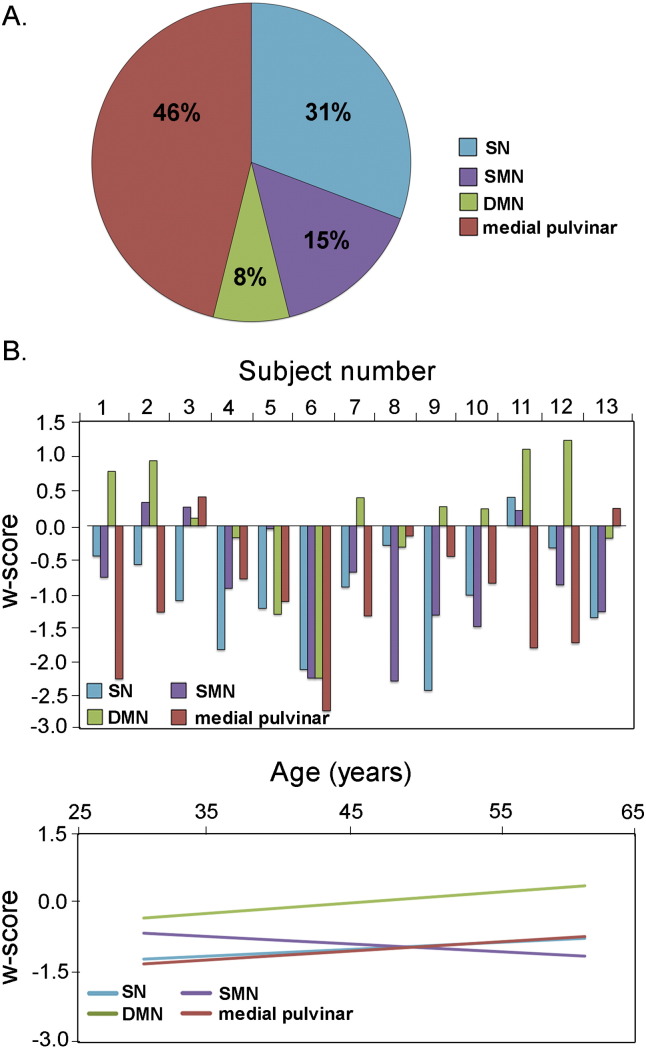
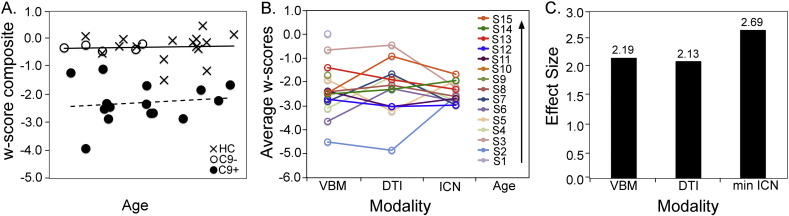
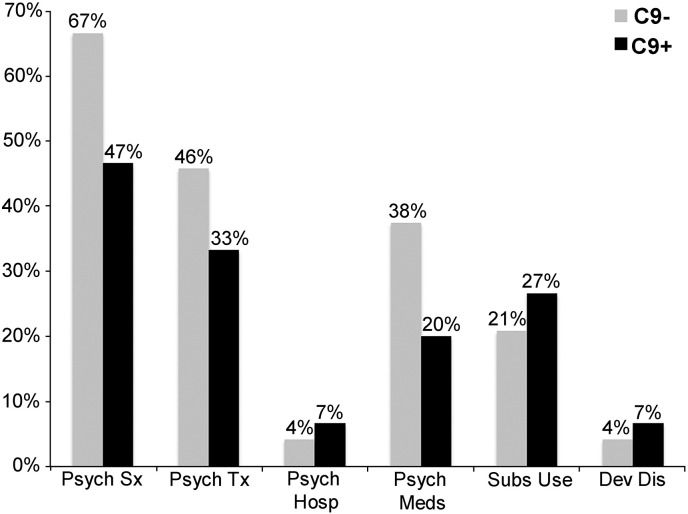
Hexanucleotide repeat expansions in C9ORF72 are the most common known genetic cause of familial and sporadic frontotemporal dementia and amyotrophic lateral sclerosis. Previous work has shown that patients with behavioral variant frontotemporal dementia due to C9ORF72 show salience and sensorimotor network disruptions comparable to those seen in sporadic behavioral variant frontotemporal dementia, but it remains unknown how early in the lifespan these and other changes in brain structure and function arise. To gain insights into this question, we compared 15 presymptomatic carriers (age 43.7 ± 10.2 years, nine females) to matched healthy controls. We used voxel-based morphometry to assess gray matter, diffusion tensor imaging to interrogate white matter tracts, and task-free functional MRI to probe the salience, sensorimotor, default mode, and medial pulvinar thalamus-seeded networks. We further used a retrospective chart review to ascertain psychiatric histories in carriers and their non-carrier family members. Carriers showed normal cognition and behavior despite gray matter volume and brain connectivity deficits that were apparent as early as the fourth decade of life. Gray matter volume deficits were topographically similar though less severe than those in patients with behavioral variant frontotemporal dementia due to C9ORF72, with major foci in cingulate, insula, thalamus, and striatum. Reduced white matter integrity was found in the corpus callosum, cingulum bundles, corticospinal tracts, uncinate fasciculi and inferior longitudinal fasciculi. Intrinsic connectivity deficits were detected in all four networks but most prominent in salience and medial pulvinar thalamus-seeded networks. Carrier and control groups showed comparable relationships between imaging metrics and age, suggesting that deficits emerge during early adulthood. Carriers and non-carrier family members had comparable lifetime histories of psychiatric symptoms. Taken together, the findings suggest that presymptomatic C9ORF72 expansion carriers exhibit functionally compensated brain volume and connectivity deficits that are similar, though less severe, to those reported during the symptomatic phase. The early adulthood emergence of these deficits suggests that they represent aberrant network patterning during development, an early neurodegeneration prodrome, or both.
Keywords: ALS, amyotrophic lateral sclerosis; Amyotrophic lateral sclerosis; CDR, Clinical Dementia Rating scale; DMN, default mode network; Diffusion tensor imaging; FA, fractional anisotropy; FTD, frontotemporal dementia; FWE, familywise error; Frontotemporal dementia; Functional MRI; Genetics; HC, healthy control; ICN, intrinsic connectivity network; IRI, Interpersonal Reactivity Index; MMSE, Mini-Mental State Exam; MND, motor neuron disease; NPI, Neuropsychiatric Inventory; ROI, region of interest; SMN, sensorimotor network; TIV, total intracranial volume; VBM, voxel-based morphometry; bvFTD, behavioral variant frontotemporal dementia; fMRI, functional MRI; preSxC9, presymptomatic C9ORF72 expansion carriers.
Figures
References
-
- Benarroch E.E. Pulvinar: associative role in cortical function and clinical correlations. Neurology. 2015;84:738–747. - PubMed
-
- Boeve B.F., Boylan K.B., Graff-Radford N.R., DeJesus-Hernandez M., Knopman D.S., Pedraza O., Vemuri P., Jones D., Lowe V., Murray M.E., Dickson D.W., Josephs K.A., Rush B.K., Machulda M.M., Fields J.A., Ferman T.J., Baker M., Rutherford N.J., Adamson J., Wszolek Z.K., Adeli A., Savica R., Boot B., Kuntz K.M., Gavrilova R., Reeves A., Whitwell J., Kantarci K., Jack C.R., Parisi J.E., Lucas J.A., Petersen R.C., Rademakers R. Characterization of frontotemporal dementia and/or amyotrophic lateral sclerosis associated with the GGGGCC repeat expansion in C9ORF72. Brain. 2012;135:765–783. - PMC - PubMed
-
- Bora E., Fornito A., Yücel M., Pantelis C. Vol. 67. BPS; 2010. Voxelwise Meta-Analysis of Gray Matter Abnormalities in Bipolar Disorder; pp. 1097–1105. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
