

Caudal Epidural Block: An Updated Review of Anatomy and Techniques
- PMID: 28337460
- PMCID: PMC5346404
- DOI: 10.1155/2017/9217145
Caudal Epidural Block: An Updated Review of Anatomy and Techniques
Abstract
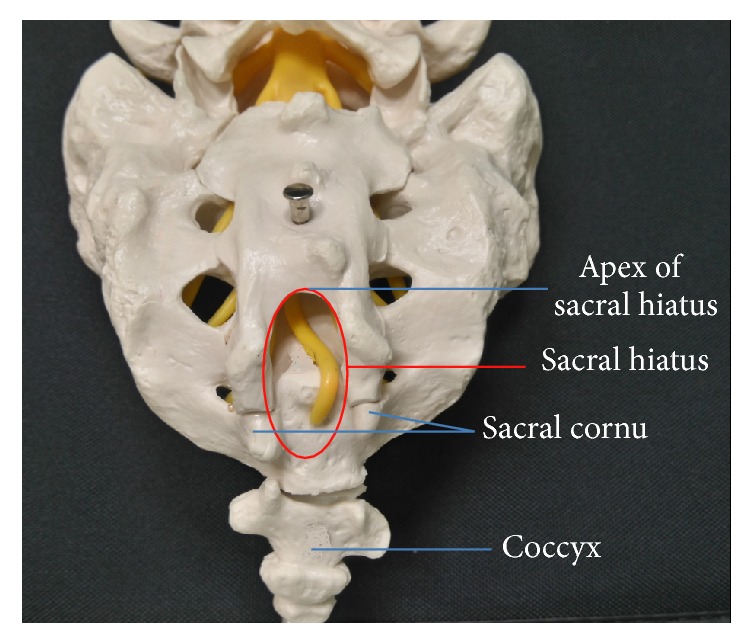
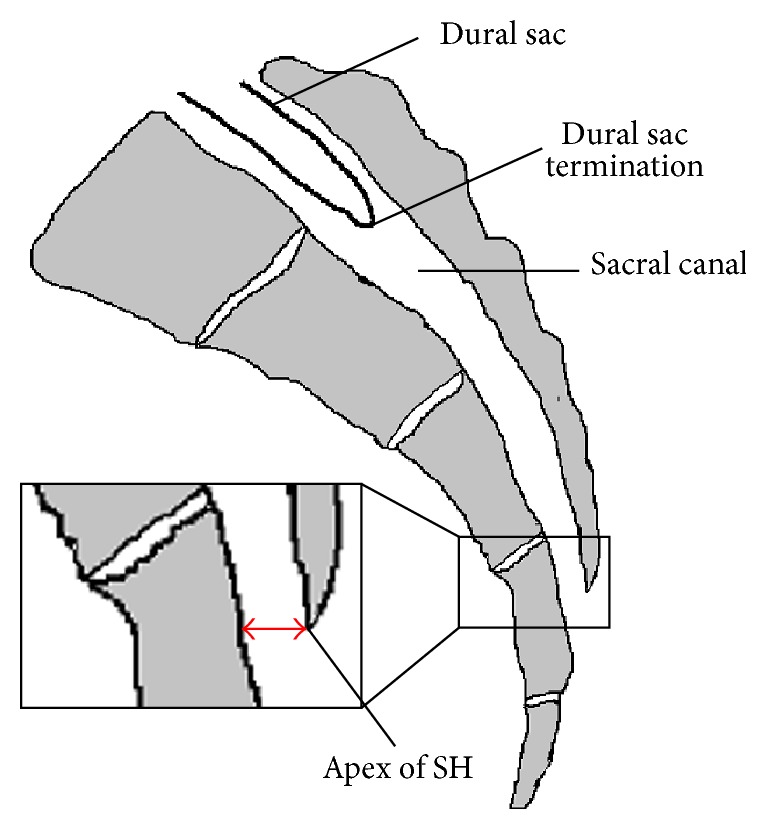
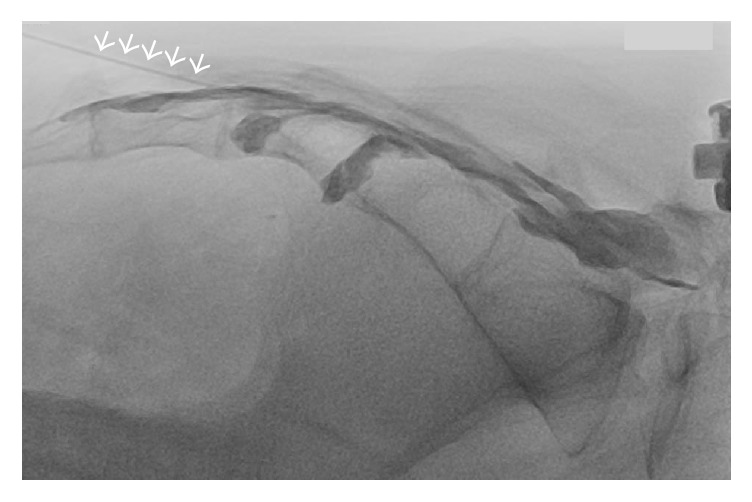
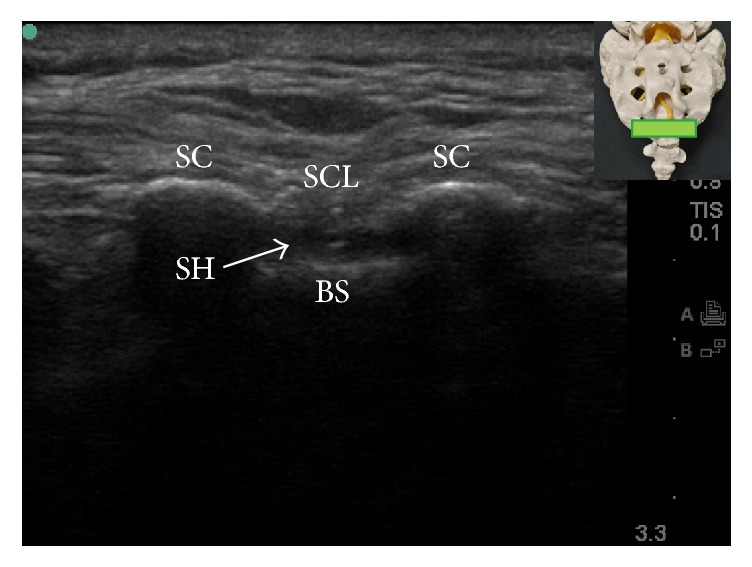
Caudal epidural block is a commonly used technique for surgical anesthesia in children and chronic pain management in adults. It is performed by inserting a needle through the sacral hiatus to gain entrance into the sacral epidural space. Using conventional blind technique, the failure rate of caudal epidural block in adults is high even in experienced hands. This high failure rate could be attributed to anatomic variations that make locating sacral hiatus difficult. With the advent of fluoroscopy and ultrasound in guiding needle placement, the success rate of caudal epidural block has been markedly improved. Although fluoroscopy is still considered the gold standard when performing caudal epidural injection, ultrasonography has been demonstrated to be highly effective in accurately guiding the needle entering the caudal epidural space and produce comparative treatment outcome as fluoroscopy. Except intravascular and intrathecal injection, ultrasonography could be as effective as fluoroscopy in preventing complications during caudal epidural injection. The relevant anatomy and techniques in performing the caudal epidural block will be briefly reviewed in this article.
Conflict of interest statement
The authors declare that there is no conflict of interests regarding the publication of this paper.
Figures
References
-
- Orme R. M., Berg S. J. The ‘swoosh’ test—an evaluation of a modified ‘whoosh’ test in children. British Journal of Anaesthesia. 2003;90:62–65. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
