

What Factors Are Associated With Femoral Component Internal Rotation in TKA Using the Gap Balancing Technique?
- PMID: 28337656
- PMCID: PMC5498379
- DOI: 10.1007/s11999-017-5319-4
What Factors Are Associated With Femoral Component Internal Rotation in TKA Using the Gap Balancing Technique?
Abstract
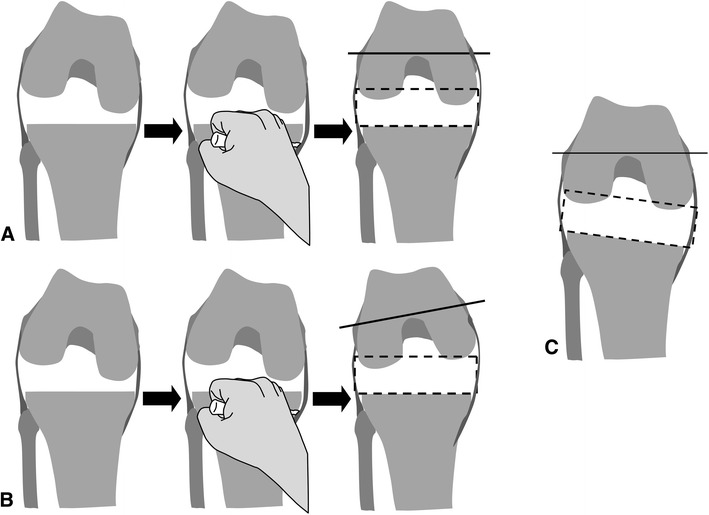
Background: When using the gap-balancing technique for TKA, excessive medial release and varus proximal tibial resection can be associated with internal rotation of the femoral component. Previous studies have evaluated the causes of femoral component rotational alignment with a separate factor analysis using unadjusted statistical methods, which might result in treatment effects being attributed to confounding variables.
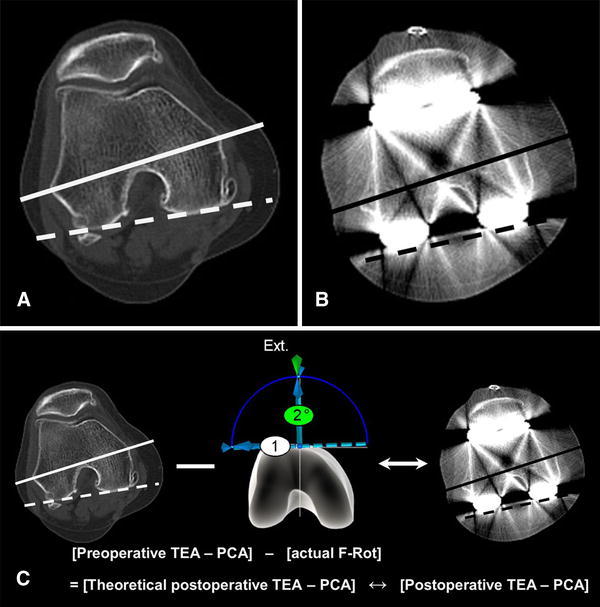
Questions/purposes: (1) What pre- and intraoperative factors are associated with internal rotation of the femoral component in TKA using the gap balancing technique? (2) To what degree does femoral component rotation as defined by the navigation system differ from rotation as measured by postoperative CT?
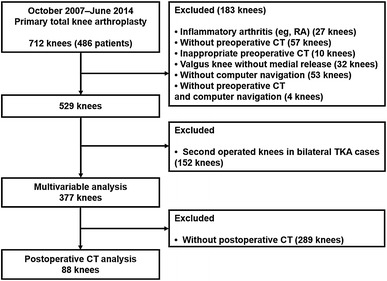
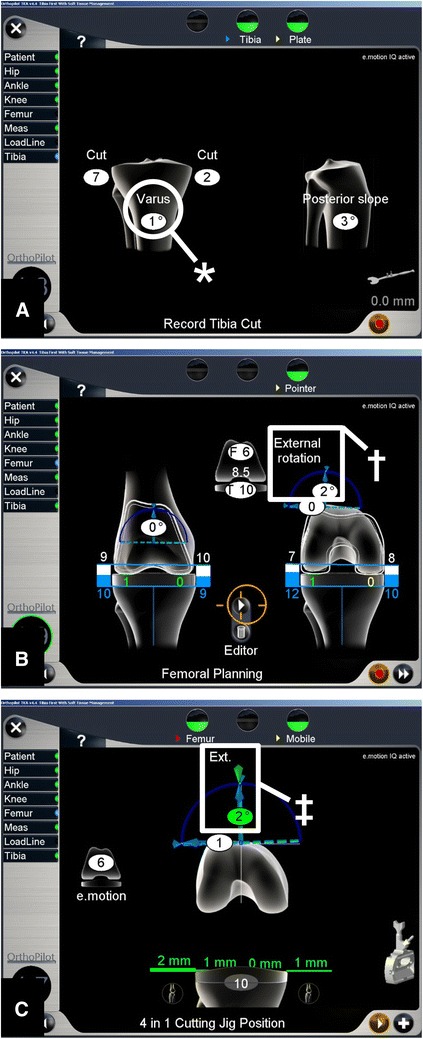
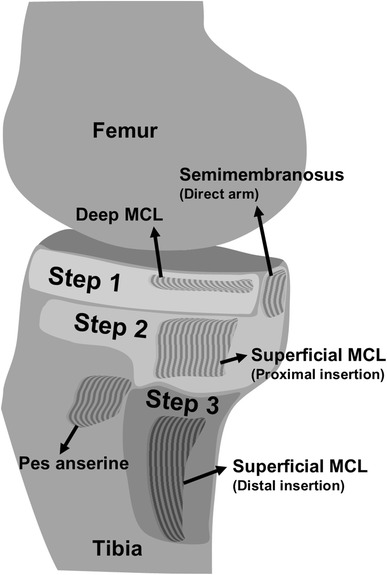
Methods: Three hundred seventy-seven knees that underwent computer-assisted primary TKA attributable to degenerative osteoarthritis with varus or mild valgus alignment in which medial soft tissue release was performed, and those with preoperative radiographs including preoperative CT between October 2007 and June 2014 were included in the study. To achieve a balanced mediolateral gap, the structures released during each medial release step were as follows: Step 1, deep medial collateral ligament (MCL); Step 2, superficial MCL (proximal, above the pes anserine tendon) and semimembranosus tendon; and Step 3, the superficial MCL (distal, below the pes anserine tendon). Knees with internal rotation of the femoral component, which was directed by navigation, to achieve a rectangular mediolateral flexion gap were considered cases, and knees without internally rotated femoral components were considered controls. Univariable analysis of the variables (age, sex, BMI, operated side, preoperative hip-knee-ankle angle, preoperative medial proximal tibial angle, preoperative rotation degree of the clinical transepicondylar axis [TEA] relative to the posterior condylar axis [PCA], coronal angle of resected tibia, resection of the posterior cruciate ligament, type of prosthesis, and extent of medial release) of cases and controls was performed, followed by a multivariable logistic regression analysis on those factors where p equals 0.15 or less. For an evaluation of navigation error, 88 knees that underwent postoperative CT were analyzed. Postoperative CT scans were obtained for patients with unexplained pain or stiffness after the operations. Using the paired t-test and Pearson's correlation analysis, the postoperative TEA-PCA measured with postoperative CT was compared with theoretical TEA-PCA, which was calculated with preoperative TEA-PCA and actual femoral component rotation checked by the navigation system.
Results: After controlling for a relevant confounding variable such as postoperative hip-knee-ankle angle, we found that the extent of medial release (Step 1 as reference; Step 2: odds ratio [OR], 5.7, [95% CI, 2.2-15]; Step 3: OR, 22, [95% CI, 7.8-62], p < 0.001) was the only factor we identified that was associated with internal rotation of the femoral component. With the numbers available, we found no difference between the mean theoretical postoperative TEA-PCA and the postoperative TEA-PCA measured using postoperative CT (4.8° ± 2.7º versus 5.0° ± 2.3º; mean difference, 0.2° ± 1.5º; p = 0.160).
Conclusions: Extent of medial release was the only factor we identified that was associated with internal rotation of the femoral component in gap-balancing TKA. To avoid internal rotation of the femoral component, we recommend a carefully subdivided medial-releasing technique, especially for the superficial MCL because once the superficial MCL has been completely released it cannot easily be restored.
Level of evidence: Level III, therapeutic study.
Figures
References
-
- Altman DG. Practical Statistics for Medical Research. 1. London, UK: Chapman & Hall; 1991.
-
- Bellemans J. Multiple needle puncturing: balancing the varus knee. Orthopedics. 2011;34:e510–e512. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
