

Acquired pulmonary artery pseudoaneurysms: a pictorial review
- PMID: 28337922
- PMCID: PMC5602174
- DOI: 10.1259/bjr.20160783
Acquired pulmonary artery pseudoaneurysms: a pictorial review
Abstract
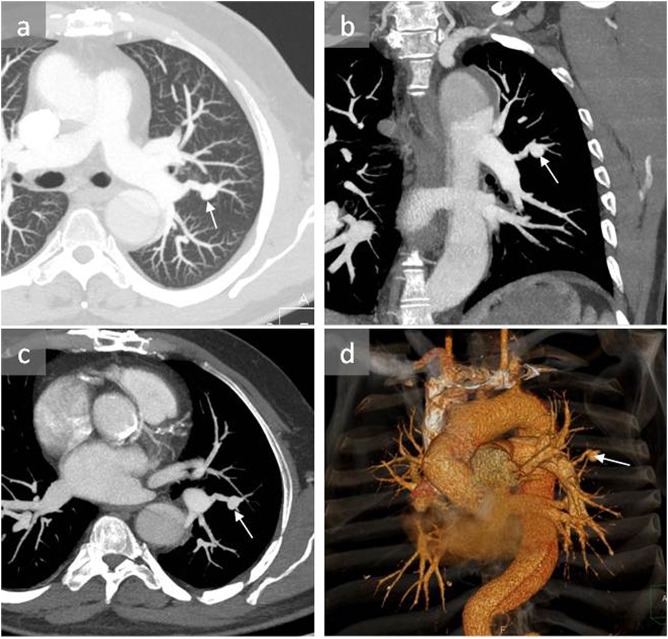
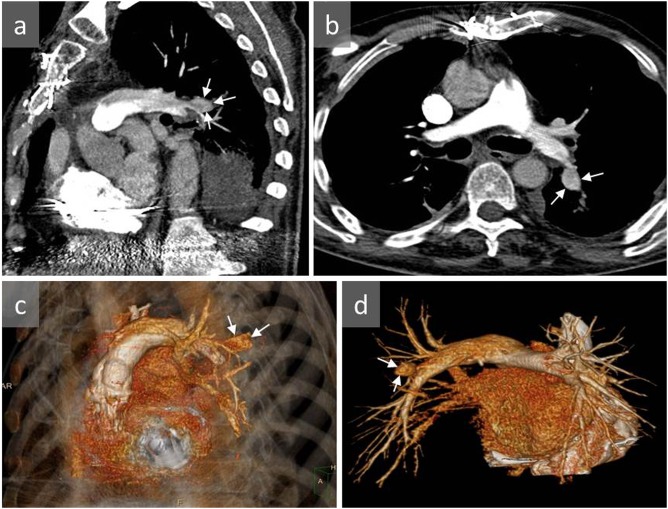
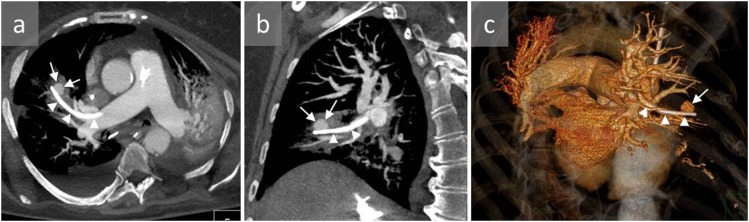
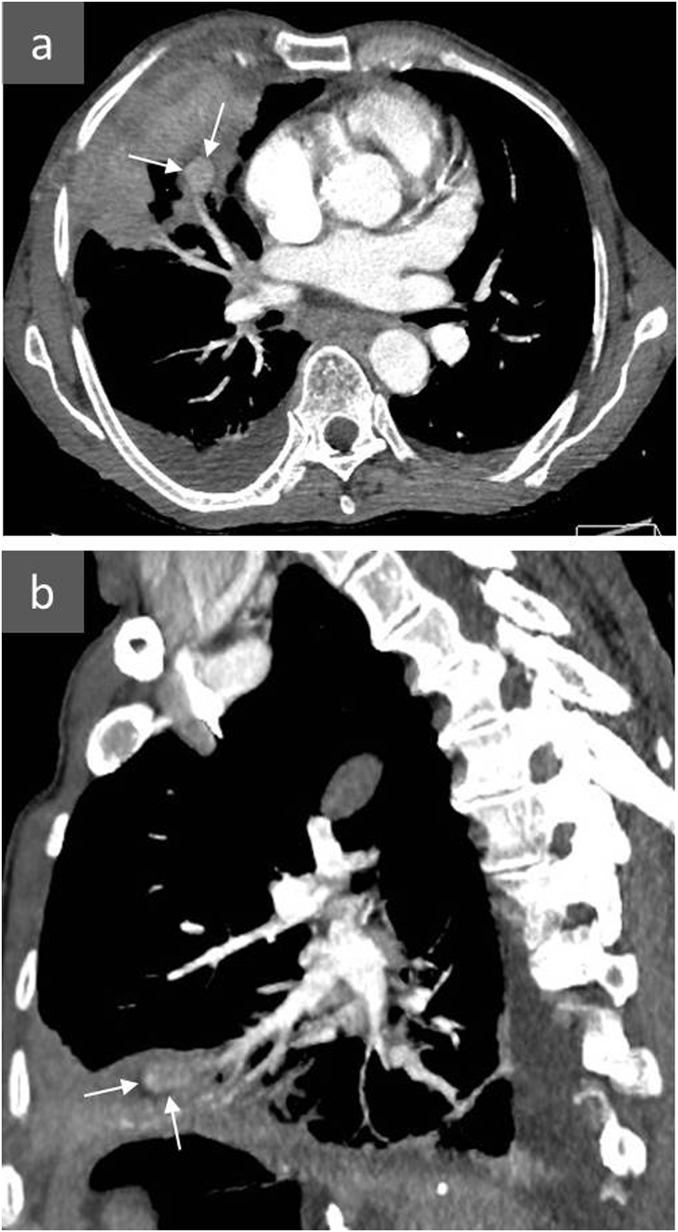
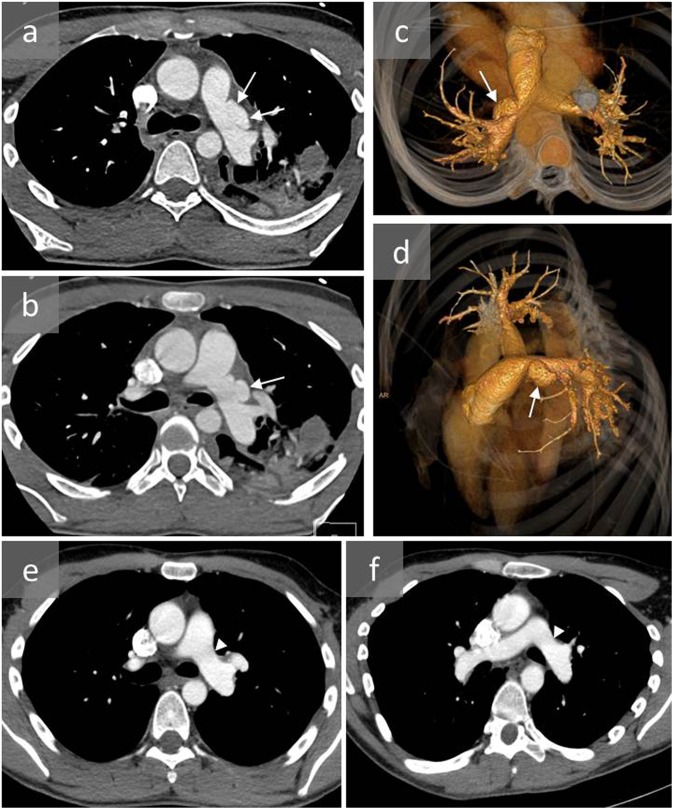
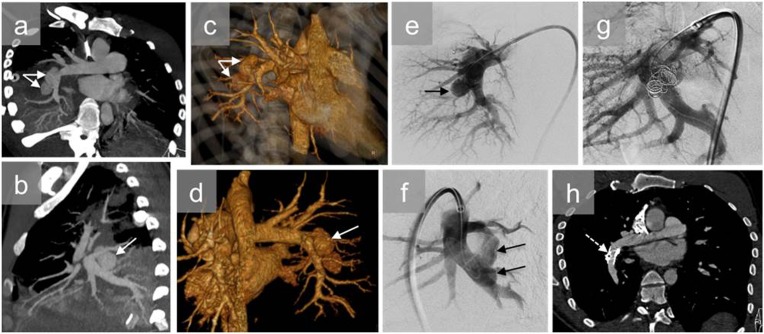
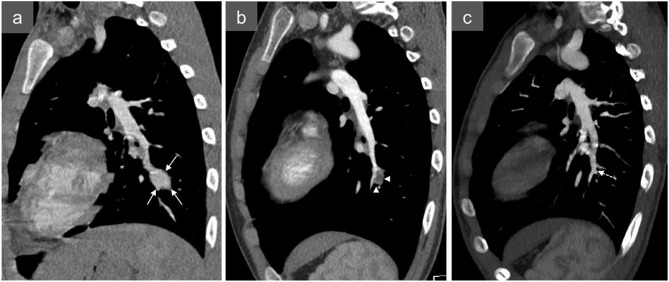
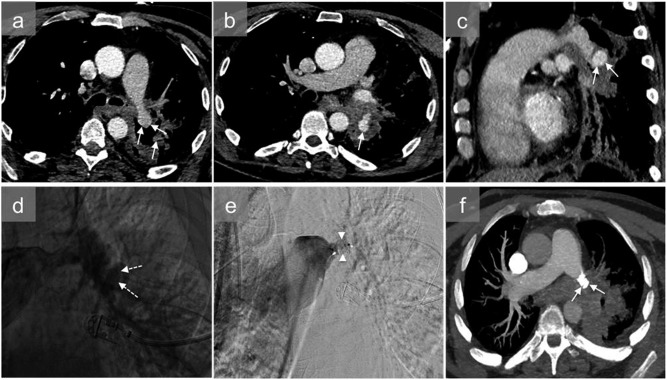
Pulmonary artery pseudoaneurysms (PAPs) are uncommon but potentially lethal. They may be incidentally discovered on imaging, or following massive haemoptysis if they rupture, with high risk of mortality. The most frequent causes of PAP are trauma and infectious disease. Vasculitis, in particular Behçet's disease, neoplasm, congenital disease and pulmonary hypertension are rarer causes of PAP. A PAP can be suspected from chest X-ray and contrast CT, but requires confirmation by CT angiography. Arteriography is no longer performed for diagnostic purposes, but can be useful in preparing endovascular occlusion of the PAP. In rare cases, surgery is necessary. The aim of this pictorial review was to illustrate the most common causes of acquired PAPs.
Figures


References
-
- Shuaib W, Tiwana MH, Vijayasarathi A, Sadiq MF, Anderson S, Amin N, et al. Imaging of vascular pseudoaneurysms in the thorax and abdomen. Clin Imaging 2015; 39: 352–62. doi: https://doi.org/10.1016/j.clinimag.2015.01.013 - DOI - PubMed
-
- Theodoropoulos P, Ziganshin BA, Tranquilli M, Elefteriades JA. Pulmonary artery aneurysms: four case reports and literature review. Int J Angiol 2013; 22: 143–8. doi: https://doi.org/10.1055/s-0033-1347907 - DOI - PMC - PubMed
-
- Duijnhouwer AL, Navarese EP, Van Dijk AP, Loeys B, Roos-Hesselink JW, De Boer MJ. Aneurysm of the pulmonary artery, a systematic review and critical analysis of current literature. Congenit Heart Dis 2016; 11: 102–9. doi: https://doi.org/10.1111/chd.12316 - DOI - PubMed
-
- Pelage JP, El Hajjam M, Lagrange C, Chinet T, Vieillard-Baron A, Chagnon S, et al. Pulmonary artery interventions: an overview. RadioGraphics 2005; 25: 1653–67. doi: https://doi.org/10.1148/rg.256055516 - DOI - PubMed
-
- Shin TB, Yoon SK, Lee KN, Choi JS, Kim YH, Sung CG, et al. The role of pulmonary CT angiography and selective pulmonary angiography in endovascular management of pulmonary artery pseudoaneurysms associated with infectious lung diseases. J Vasc Interv Radiol 2007; 18: 882–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
