

Integrative Blood Pressure Response to Upright Tilt Post Renal Denervation
- PMID: 28338768
- PMCID: PMC5861553
- DOI: 10.1093/ajh/hpx018
Integrative Blood Pressure Response to Upright Tilt Post Renal Denervation
Abstract
Background: Whether renal denervation (RDN) in patients with resistant hypertension normalizes blood pressure (BP) regulation in response to routine cardiovascular stimuli such as upright posture is unknown. We conducted an integrative study of BP regulation in patients with resistant hypertension who had received RDN to characterize autonomic circulatory control.
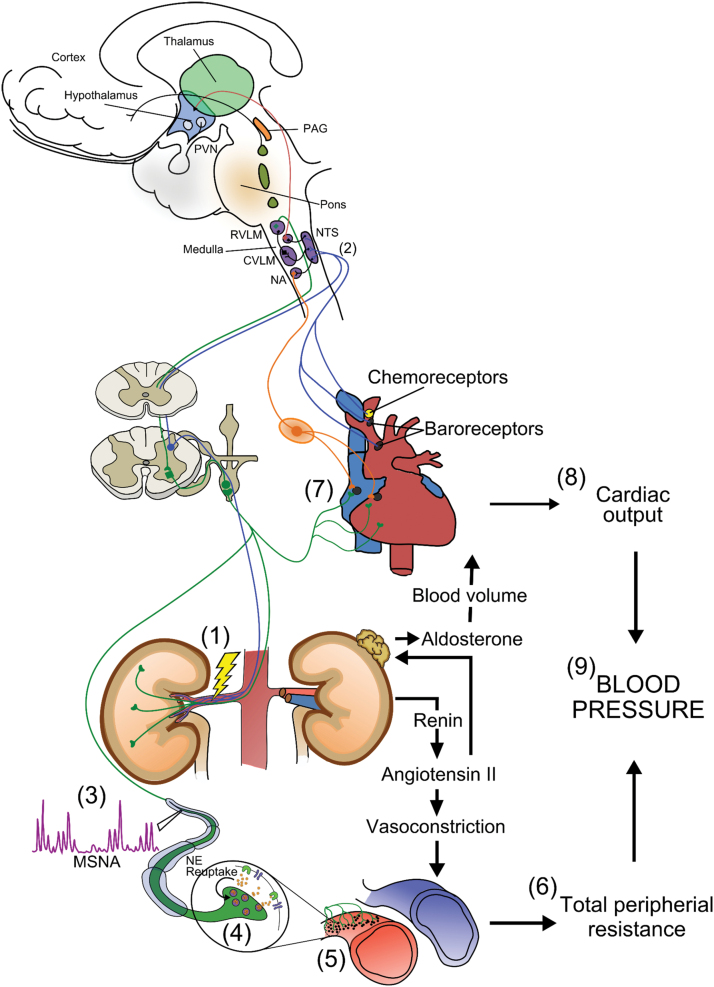
Methods: Twelve patients (60 ± 9 [SD] years, n = 10 males) who participated in the Symplicity HTN-3 trial were studied and compared to 2 age-matched normotensive (Norm) and hypertensive (unmedicated, HTN) control groups. BP, heart rate (HR), cardiac output (Qc), muscle sympathetic nerve activity (MSNA), and neurohormonal variables were measured supine, and 30° (5 minutes) and 60° (20 minutes) head-up-tilt (HUT). Total peripheral resistance (TPR) was calculated from mean arterial pressure and Qc.
Results: Despite treatment with RDN and 4.8 (range, 3-7) antihypertensive medications, the RDN had significantly higher supine systolic BP compared to Norm and HTN (149 ± 15 vs. 118 ± 6, 108 ± 8 mm Hg, P < 0.001). When supine, RDN had higher HR, TPR, MSNA, plasma norepinephrine, and effective arterial elastance compared to Norm. Plasma norepinephrine, Qc, and HR were also higher in the RDN vs. HTN. During HUT, BP remained higher in the RDN, due to increases in Qc, plasma norepinephrine, and aldosterone.
Conclusion: We provide evidence of a possible mechanism by which BP remains elevated post RDN, with the observation of increased Qc and arterial stiffness, as well as plasma norepinephrine and aldosterone levels at approximately 2 years post treatment. These findings may be the consequence of incomplete ablation of sympathetic renal nerves or be related to other factors.
Keywords: ablation; autonomic nervous system; blood pressure; human; hypertension; physiology; sympathetic activity.
© American Journal of Hypertension, Ltd 2017. All rights reserved. For Permissions, please email: journals.permissions@oup.com
Figures



Similar articles
-
Renal Sympathetic Denervation: A Viable Option for Treating Resistant Hypertension.Am J Hypertens. 2017 Sep 1;30(9):847-856. doi: 10.1093/ajh/hpx033. Am J Hypertens. 2017. PMID: 28338871 Review.
-
Blood pressure changes after catheter-based renal denervation are related to reductions in total peripheral resistance.J Hypertens. 2015 Dec;33(12):2519-25. doi: 10.1097/HJH.0000000000000752. J Hypertens. 2015. PMID: 26485463
-
Orthostatic function after renal sympathetic denervation in patients with resistant hypertension.Int J Cardiol. 2013 Nov 30;169(6):418-24. doi: 10.1016/j.ijcard.2013.10.017. Epub 2013 Oct 12. Int J Cardiol. 2013. PMID: 24157238
-
Effects of catheter-based renal denervation on cardiac sympathetic activity and innervation in patients with resistant hypertension.Clin Res Cardiol. 2016 Apr;105(4):364-71. doi: 10.1007/s00392-015-0930-4. Epub 2015 Oct 22. Clin Res Cardiol. 2016. PMID: 26493305
-
Resistant Hypertension and Renal Nerve Denervation.Methodist Debakey Cardiovasc J. 2015 Oct-Dec;11(4):240-4. doi: 10.14797/mdcj-11-4-240. Methodist Debakey Cardiovasc J. 2015. PMID: 27057294 Free PMC article. Review.
References
-
- Calhoun DA, Jones D, Textor S, Goff DC, Murphy TP, Toto RD, White A, Cushman WC, White W, Sica D, Ferdinand K, Giles TD, Falkner B, Carey RM; American Heart Association Professional Education Committee. Resistant hypertension: diagnosis, evaluation, and treatment: a scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Circulation 2008; 117:e510–e526. - PubMed
-
- Sarafidis PA, Georgianos P, Bakris GL. Resistant hypertension–its identification and epidemiology. Nat Rev Nephrol 2013; 9:51–58. - PubMed
-
- DiBona GF, Esler M. Translational medicine: the antihypertensive effect of renal denervation. Am J Physiol Regul Integr Comp Physiol 2010; 298:R245–R253. - PubMed
-
- Krum H, Schlaich M, Whitbourn R, Sobotka PA, Sadowski J, Bartus K, Kapelak B, Walton A, Sievert H, Thambar S, Abraham WT, Esler M. Catheter-based renal sympathetic denervation for resistant hypertension: a multicentre safety and proof-of-principle cohort study. Lancet 2009; 373:1275–1281. - PubMed
-
- DiBona GF, Kopp UC. Neural control of renal function. Physiol Rev 1997; 77:75–197. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
