

Reducing Antimicrobial Use in an Academic Pediatric Institution: Evaluation of the Effectiveness of a Prospective Audit With Real-Time Feedback
- PMID: 28339590
- PMCID: PMC5907874
- DOI: 10.1093/jpids/piw054
Reducing Antimicrobial Use in an Academic Pediatric Institution: Evaluation of the Effectiveness of a Prospective Audit With Real-Time Feedback
Abstract
Introduction: Antimicrobial use is decreasing across freestanding children's hospitals, predominantly in institutions with antimicrobial stewardship programs (ASPs) in place. A highly effective ASP should effect a greater decrease in use than predicted by existing trends. Antimicrobial stewardship programs depend on clinician adherence to program recommendations, but little is known about factors associated with adherence.
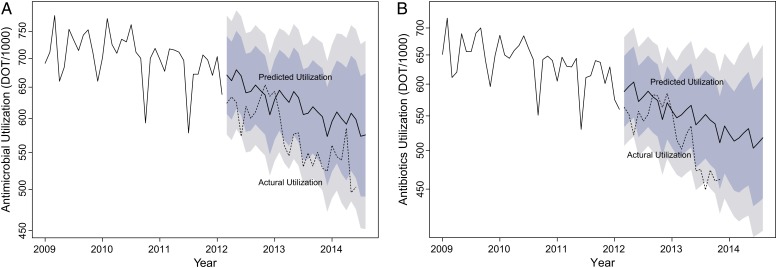
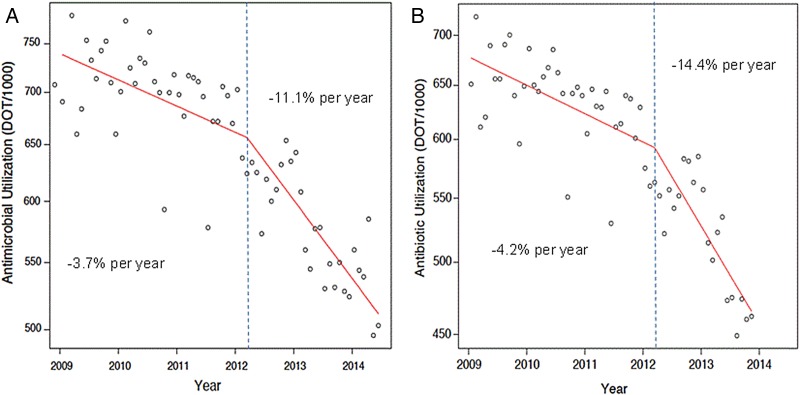
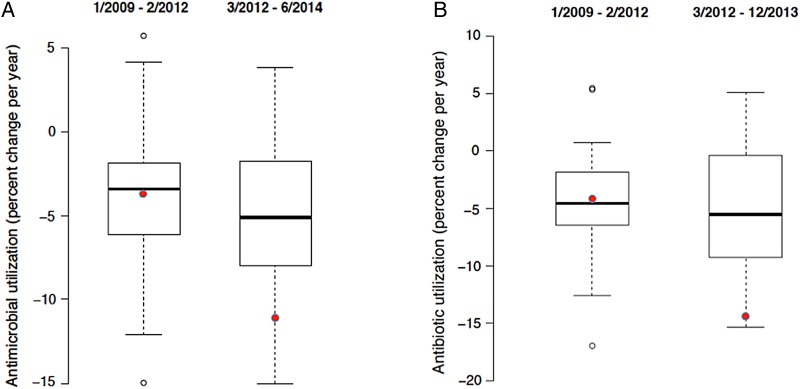
Methods: Parenteral antimicrobial-use data for our institution and 43 additional freestanding children's hospitals were obtained and normalized for patient census. Segmental linear regression was used to compare rates of change of parenteral antimicrobial use before and after ASP implementation. Time-series models were developed to predict use in the absence of intervention. The odds of adherence to ASP recommendations were determined based on provider characteristics and recommendation type.
Results: In the 38 months before ASP implementation, parenteral antimicrobial use was decreasing at our hospital by 3.7%/year, similar to the 3.4%/year found across children's hospitals. The rate of change after implementation of the ASP at our hospital was 11.1%/year, compared to 5.6%/year for other hospitals over the same period. Of 643 interventions, teams adhered with recommendations in 495 cases (77.0%). According to adjusted analysis, primary service was not associated with adherence (P = .356). There was an association between adherence and the role of the clinician receiving a recommendation (P = .009) and the recommendation type (P = .009).
Conclusions: Understanding factors associated with adherence to ASP recommendations can help those who administer such programs to strategize interventions for maximizing efficacy. Our findings reveal the value of a formal ASP in reducing use when controlling for secular trends.
Keywords: antimicrobial stewardship; antimicrobial utilization; cost-effectiveness.
© The Author 2016. Published by Oxford University Press on behalf of the Pediatric Infectious Diseases Society. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Di Pentima MC, Chan S, Eppes SC, Klein JD. Antimicrobial prescription errors in hospitalized children: role of antimicrobial stewardship program in detection and intervention. Clin Pediatr (Phila) 2009; 48:505–12. - PubMed
-
- John JF, Fishman NO. Programmatic role of the infectious diseases physician in controlling antimicrobial costs in the hospital. Clin Infect Dis 1997; 24:471–85. - PubMed
-
- Schentag JJ, Ballow CH, Fritz AL et al. . Changes in antimicrobial agent usage resulting from interactions among clinical pharmacy, the infectious disease division, and the microbiology laboratory. Diagn Microbiol Infect Dis 1993; 16:255–64. - PubMed
-
- Ansari F, Gray K, Nathwani D et al. . Outcomes of an intervention to improve hospital antibiotic prescribing: interrupted time series with segmented regression analysis. J Antimicrob Chemother 2003; 52:842–8. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
