

Clinical treatment considerations in the intensity-modulated radiotherapy era for patients with N0-category nasopharyngeal carcinoma and enlarged neck lymph nodes
- PMID: 28340596
- PMCID: PMC5364609
- DOI: 10.1186/s40880-017-0199-2
Clinical treatment considerations in the intensity-modulated radiotherapy era for patients with N0-category nasopharyngeal carcinoma and enlarged neck lymph nodes
Abstract
Background: Nasopharyngeal carcinoma (NPC) shows a high proportion of lymph node metastasis, and treatment guidelines have been developed for positive nodes. However, no irradiation guidelines have been proposed for patients with enlarged neck lymph nodes (ENLNs) that do not meet the radiological criteria of 10 mm in diameter for positive lymph nodes. This study aimed to determine the prognostic value and radiation dose for ENLNs in N0-category NPC patients treated with intensity-modulated radiotherapy (IMRT).
Methods: We reviewed the medical data of 251 patients with non-metastatic, N0-category NPC treated with IMRT. Receiver operating characteristic curves were used to calculate the cut-off value of the ENLN diameter for the prediction of disease failure. The biological equivalent dose (BED) for ENLNs was calculated. Patient survival was compared between the small and large ENLN groups. Independent prognostic factors were identified using the Cox proportional hazards model.
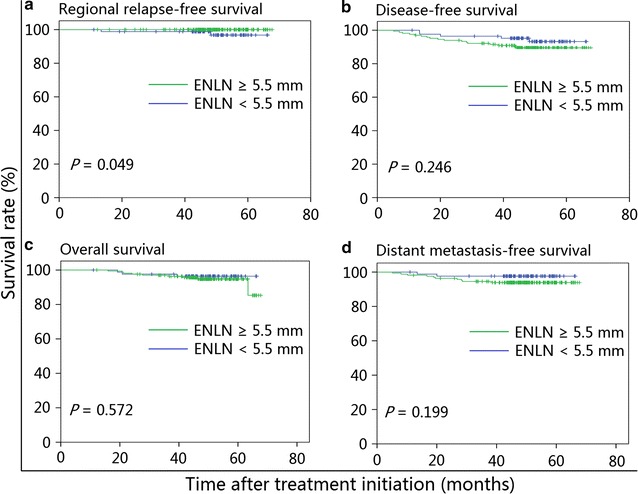
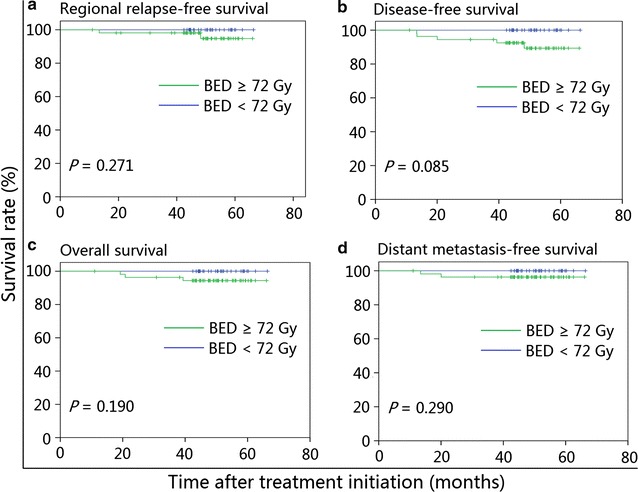
Results: The estimated 4-year regional relapse-free survival rate was higher in patients with ENLNs ≥5.5 mm than in those with ENLNs <5.5 mm (100% vs. 98.8%, P = 0.049), whereas disease-free, overall, and distant metastasis-free survival rates were similar between the two groups. After adjusting for various factors, ENLN diameter was not identified as an independent prognostic factor (P > 0.05 for all survival rates). In the subgroup analysis, patients receiving BED ≥72 Gy had a similar prognosis as patients receiving BED <72 Gy in both the small and large ENLN groups. The multivariate analysis also confirmed that BED ≥72 Gy was not associated with significantly improved prognosis in patients with N0-category NPC.
Conclusions: A BED of 72 Gy to ENLNs is considerably sufficient to provide a clinical benefit to patients with N0-category NPC. Prospective studies are warranted to validate the findings in the present study.
Keywords: Biological equivalent dose; Enlarged neck lymph node; Intensity-modulated radiotherapy; N0-category; Nasopharyngeal carcinoma; Prognosis.
Figures


References
-
- National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology, version 1.2016. http://www.nccn.org/professionals/physician_gls/f_guidelines.asp. Accessed 6 May 2016.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
