

Frequency of Left Ventricular End-Diastolic Volume-Mediated Declines in Ejection Fraction in Patients Receiving Potentially Cardiotoxic Cancer Treatment
- PMID: 28341361
- PMCID: PMC5406277
- DOI: 10.1016/j.amjcard.2017.02.008
Frequency of Left Ventricular End-Diastolic Volume-Mediated Declines in Ejection Fraction in Patients Receiving Potentially Cardiotoxic Cancer Treatment
Abstract
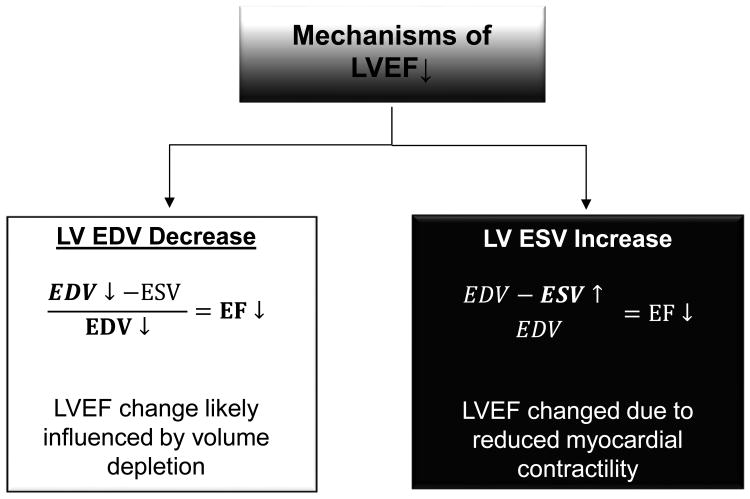
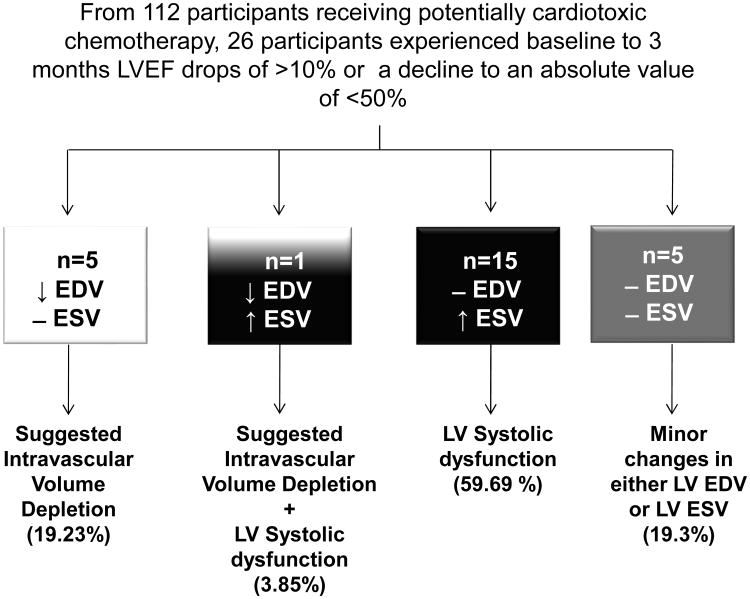
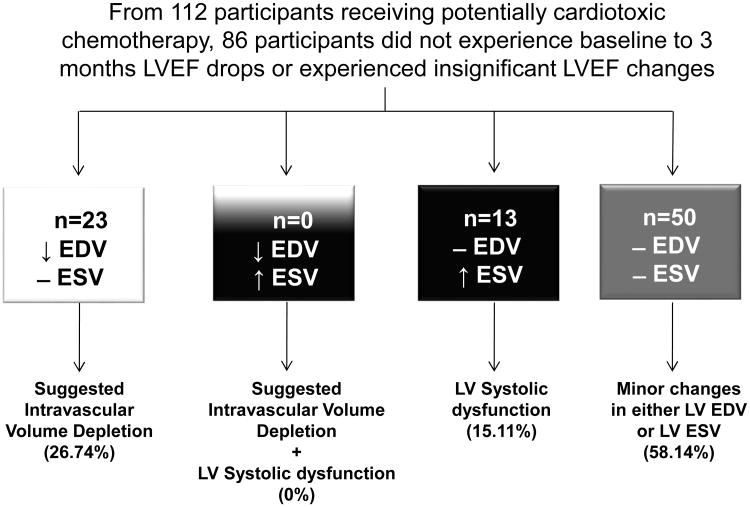
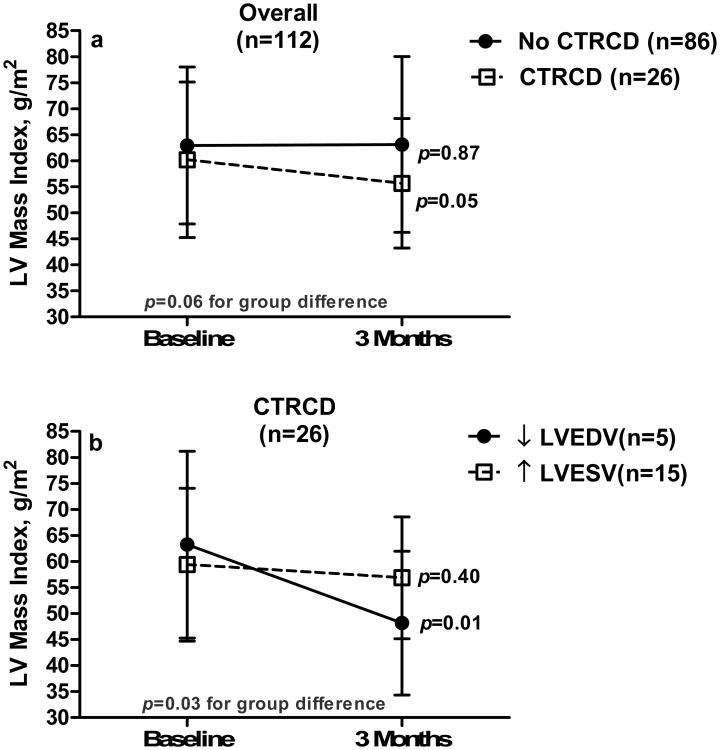
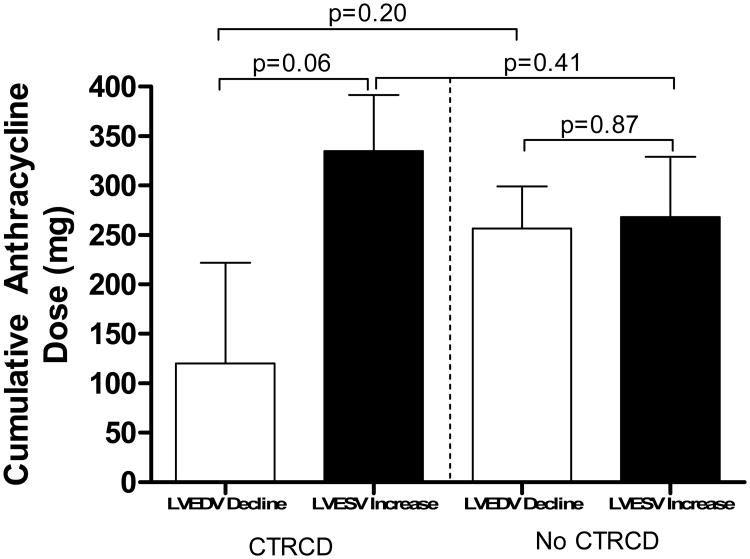
We sought to determine the frequency by which decreases in left ventricular (LV) end-diastolic volume (LVEDV) with and without increases in end-systolic volume (LVESV) influenced early cancer treatment-associated declines in LV ejection fraction (LVEF) or LV mass. One hundred twelve consecutively recruited subjects (aged 52 ± 14 years) with cancer underwent blinded cardiovascular magnetic resonance measurements of LV volumes, mass, and LVEF before and 3 months after initiating potentially cardiotoxic chemotherapy (72% of participants received anthracyclines). Twenty-six participants developed important declines in LVEF of >10% or to values <50% at 3 months, in whom 19% versus 60%, respectively, experienced their decline in LVEF due to isolated declines in LVEDV versus an increase in LVESV; participants who dropped their LVEF due to decreases in LVEDV lost more LV mass than those who dropped their LVEF due to an increase in LVESV (p = 0.03). Nearly one fifth of subjects experience marked LVEF declines due to an isolated decline in LVEDV after initiating potentially cardiotoxic chemotherapy. Because reductions in intravascular volume (which could be treated by volume repletion) may account for LVEDV-related declines in LVEF, these data indicate that LV volumes should be reviewed along with LVEF when acquiring imaging studies for cardiotoxicity during the treatment for cancer.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Drafts BC, Twomley KM, D'Agostino R, Jr, Lawrence J, Avis N, Ellis LR, Thohan V, Jordan J, Melin SA, Torti FM, Little WC, Hamilton CA, Hundley WG. Low to moderate dose anthracycline-based chemotherapy is associated with early noninvasive imaging evidence of subclinical cardiovascular disease. JACC Cardiovasc Imaging. 2013;6:877–885. - PMC - PubMed
-
- Plana JC, Galderisi M, Barac A, Ewer MS, Ky B, Scherrer-Crosbie M, Ganame J, Sebag IA, Agler DA, Badano LP, Banchs J, Cardinale D, Carver J, Cerqueira M, DeCara JM, Edvardsen T, Flamm SD, Force T, Griffin BP, Jerusalem G, Liu JE, Magalhães A, Marwick T, Sanchez LY, Sicari R, Villarraga HR, Lancellotti P. Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: a report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2014;27:911–939. - PubMed
-
- Schwartz RG, Venci N. Can serial changes of diastolic dysfunction signal incremental risk of chemotherapy-induced heart failure missed by the timing of declining LV ejection fraction? J Nucl Cardiol. 2016;23:833–836. - PubMed
-
- Lightfoot JC, D'Agostino RB, Jr, Hamilton CA, Jordan J, Torti FM, Kock ND, Jordan J, Workman S, Hundley WG. Novel approach to early detection of doxorubicin cardiotoxicity by gadolinium-enhanced cardiovascular magnetic resonance imaging in an experimental model. Circ Cardiovasc Imaging. 2010;3:550–558. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
