

Can MRI Visual Assessment Differentiate the Variants of Primary-Progressive Aphasia?
- PMID: 28341715
- PMCID: PMC7960364
- DOI: 10.3174/ajnr.A5126
Can MRI Visual Assessment Differentiate the Variants of Primary-Progressive Aphasia?
Abstract
Background and purpose: Primary-progressive aphasia is a clinically and pathologically heterogeneous condition. Nonfluent, semantic, and logopenic are the currently recognized clinical variants. The recommendations for the classification of primary-progressive aphasia have advocated variant-specific patterns of atrophy. The aims of the present study were to evaluate the sensitivity and specificity of the proposed imaging criteria and to assess the intra- and interrater reporting agreements.
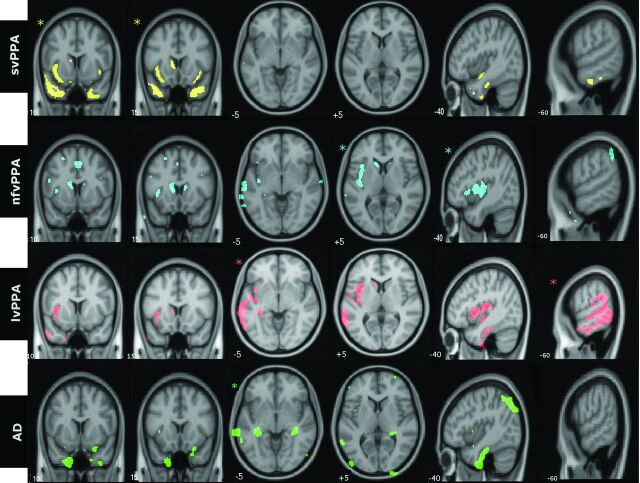
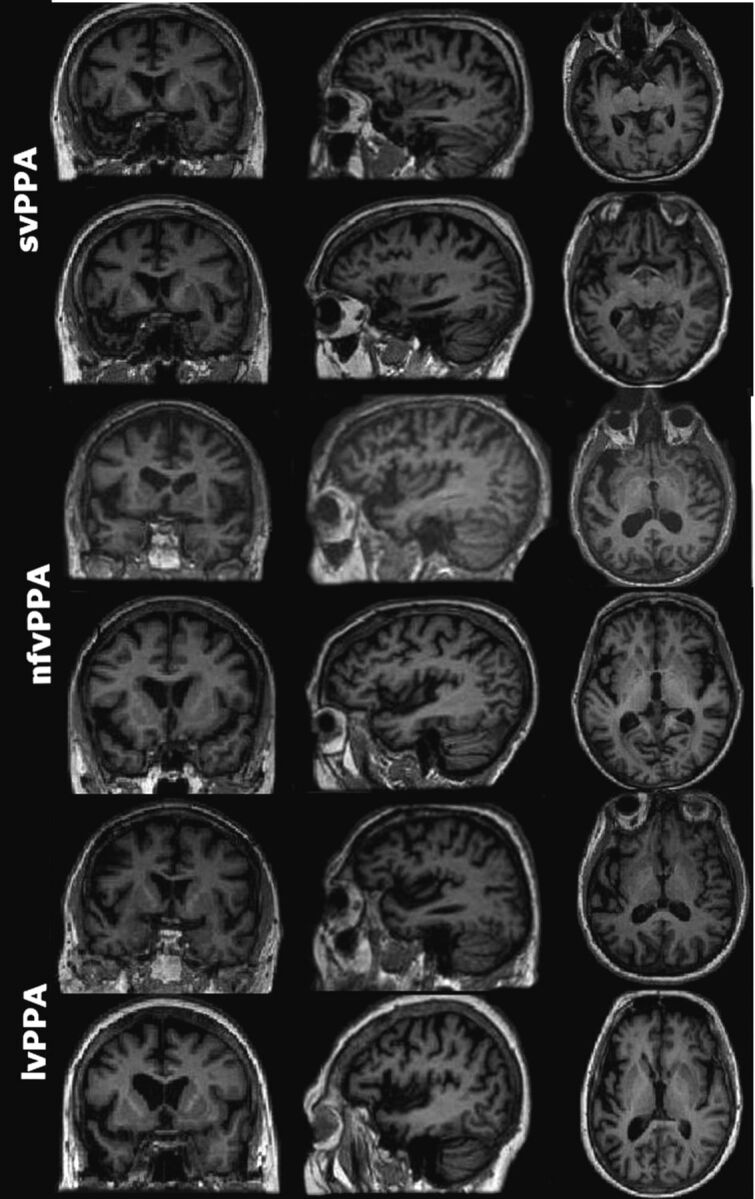
Materials and methods: The cohort comprised 51 patients with a root diagnosis of primary-progressive aphasia, 25 patients with typical Alzheimer disease, and 26 matched control participants. Group-level analysis (voxel-based morphometry) confirmed the proposed atrophy patterns for the 3 syndromes. The individual T1-weighted anatomic images were reported by 3 senior neuroradiologists.
Results: We observed a dichotomized pattern of high sensitivity (92%) and specificity (93%) for the proposed atrophy pattern of semantic-variant primary-progressive aphasia and low sensitivity (21% for nonfluent-variant primary-progressive aphasia and 43% for logopenic-variant primary-progressive aphasia) but high specificity (91% for nonfluent-variant primary-progressive aphasia and 95% for logopenic-variant primary-progressive aphasia) in other primary-progressive aphasia variants and Alzheimer disease (sensitivity 43%, specificity 92%). MR imaging was least sensitive for the diagnosis of nonfluent-variant primary-progressive aphasia. Intrarater agreement analysis showed mean κ values above the widely accepted threshold of 0.6 (mean, 0.63 ± 0.16). Pair-wise interobserver agreement outcomes, however, were well below this threshold in 5 of the 6 possible interrater contrasts (mean, 0.41 ± 0.09).
Conclusions: While the group-level results were in precise agreement with the recommendations, semantic-variant primary-progressive aphasia was the only subtype for which the proposed recommendations were both sensitive and specific at an individual level.
© 2017 by American Journal of Neuroradiology.
Figures
Comment in
-
FDG-PET/CT or MRI for the Diagnosis of Primary Progressive Aphasia?AJNR Am J Neuroradiol. 2017 Sep;38(9):E63. doi: 10.3174/ajnr.A5255. Epub 2017 May 25. AJNR Am J Neuroradiol. 2017. PMID: 28546246 Free PMC article. No abstract available.
Similar articles
-
Predicting primary progressive aphasias with support vector machine approaches in structural MRI data.Neuroimage Clin. 2017 Feb 6;14:334-343. doi: 10.1016/j.nicl.2017.02.003. eCollection 2017. Neuroimage Clin. 2017. PMID: 28229040 Free PMC article.
-
Rates of Amyloid Imaging Positivity in Patients With Primary Progressive Aphasia.JAMA Neurol. 2018 Mar 1;75(3):342-352. doi: 10.1001/jamaneurol.2017.4309. JAMA Neurol. 2018. PMID: 29309493 Free PMC article.
-
Single-word comprehension deficits in the nonfluent variant of primary progressive aphasia.Alzheimers Res Ther. 2018 Jul 18;10(1):68. doi: 10.1186/s13195-018-0393-8. Alzheimers Res Ther. 2018. PMID: 30021613 Free PMC article.
-
Validating new diagnostic imaging criteria for primary progressive aphasia via anatomical likelihood estimation meta-analyses.Eur J Neurol. 2016 Apr;23(4):704-12. doi: 10.1111/ene.12902. Epub 2016 Feb 22. Eur J Neurol. 2016. PMID: 26901360 Review.
-
Multimodality Imaging in Primary Progressive Aphasia.AJNR Am J Neuroradiol. 2022 Sep;43(9):1230-1243. doi: 10.3174/ajnr.A7613. Epub 2022 Aug 25. AJNR Am J Neuroradiol. 2022. PMID: 36007947 Free PMC article. Review.
Cited by
-
Multiparametric magnetic resonance imaging and positron emission tomography findings in neurodegenerative diseases: Current status and future directions.Neuroradiol J. 2021 Aug;34(4):263-288. doi: 10.1177/1971400921998968. Epub 2021 Mar 5. Neuroradiol J. 2021. PMID: 33666110 Free PMC article. Review.
-
Case Report: Semantic Variant of Primary Progressive Aphasia Associated With Anti-Glial Fibrillary Acid Protein Autoantibodies.Front Immunol. 2022 Jan 3;12:760021. doi: 10.3389/fimmu.2021.760021. eCollection 2021. Front Immunol. 2022. PMID: 35046935 Free PMC article.
-
Graded, multidimensional intra- and intergroup variations in primary progressive aphasia and post-stroke aphasia.Brain. 2020 Oct 1;143(10):3121-3135. doi: 10.1093/brain/awaa245. Brain. 2020. PMID: 32940648 Free PMC article.
-
Utility of visual rating scales in primary progressive aphasia.Alzheimers Res Ther. 2024 Apr 6;16(1):73. doi: 10.1186/s13195-024-01442-7. Alzheimers Res Ther. 2024. PMID: 38582927 Free PMC article.
-
FDG-PET/CT or MRI for the Diagnosis of Primary Progressive Aphasia?AJNR Am J Neuroradiol. 2017 Sep;38(9):E63. doi: 10.3174/ajnr.A5255. Epub 2017 May 25. AJNR Am J Neuroradiol. 2017. PMID: 28546246 Free PMC article. No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical