

Multiparametric Evaluation in Differentiating Glioma Recurrence from Treatment-Induced Necrosis Using Simultaneous 18F-FDG-PET/MRI: A Single-Institution Retrospective Study
- PMID: 28341716
- PMCID: PMC7960371
- DOI: 10.3174/ajnr.A5124
Multiparametric Evaluation in Differentiating Glioma Recurrence from Treatment-Induced Necrosis Using Simultaneous 18F-FDG-PET/MRI: A Single-Institution Retrospective Study
Abstract
Background and purpose: Differentiating glioma recurrence from treatment-induced necrosis can be a challenge on conventional imaging. This study aimed to assess the diagnostic performance of each functional MR imaging and PET parameter derived by using simultaneous FDG-PET/MR imaging individually and in combination in the evaluation of suspected glioma recurrence.
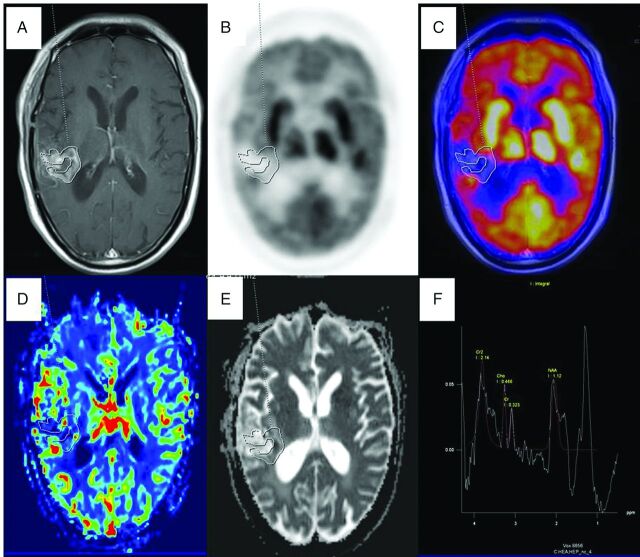
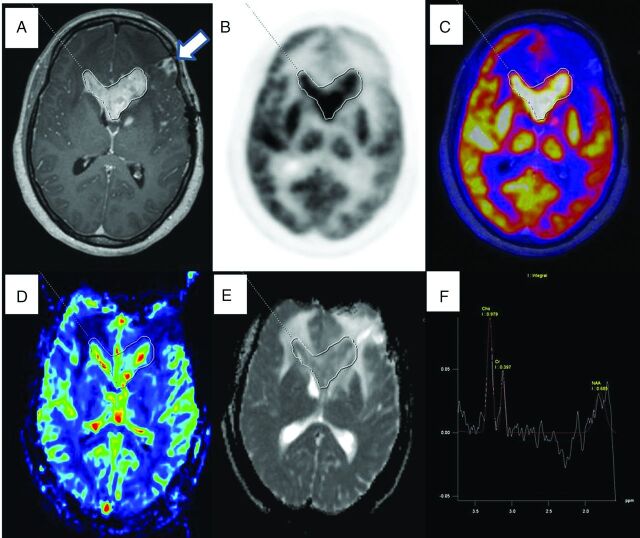
Materials and methods: Thirty-five treated glioma patients with 41 enhancing lesions (World Health Organization grade II = 9, III = 13, IV = 19) on MR imaging after an operation followed by radiation therapy and/or chemotherapy formed part of this study. Using PET/MR imaging, we calculated the normalized mean relative CBV, mean ADC, Cho/Cr, and maximum and mean target-to-background ratios. Statistical analysis was performed to determine the diagnostic performance of each parameter by receiver operating characteristic analysis individually and in combination with multivariate receiver operating characteristic analysis for the detection of glioma recurrence. Histopathology or clinicoradiologic follow-up was considered the criterion standard.
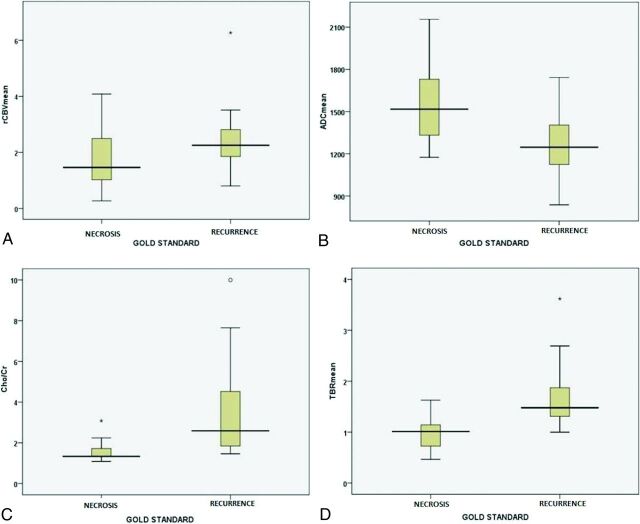
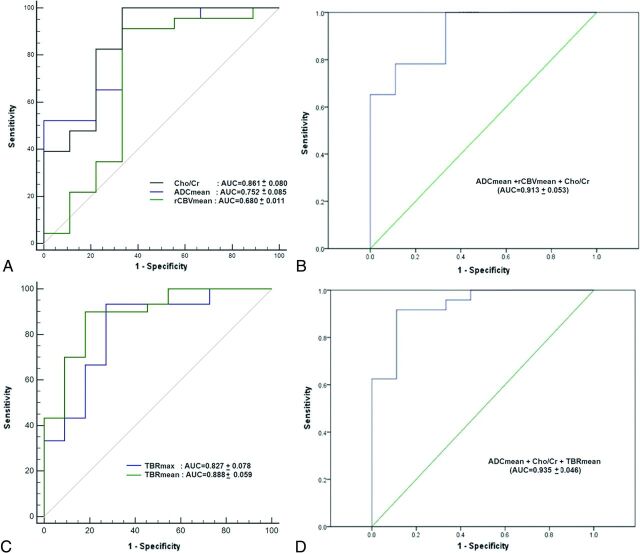
Results: Of 35 patients, 25 (30 lesions) were classified as having a recurrence and 10 (11 lesions) patients as having treatment-induced necrosis. Parameters like rCBVmean (mean relative CBV), ADCmean, Cho/Cr, and maximum and mean target-to-background ratios were statistically significant in the detection of recurrent lesions with an accuracy of 77.5%, 78.0%, 90.9%, 87.8%, and 87.8%, respectively. On multivariate receiver operating characteristic analysis, the combination of all 3 MR imaging parameters resulted in an area under the curve of 0.913 ± 0.053. Furthermore, an area under the curve of 0.935 ± 0.046 was obtained when MR imaging parameters (ADCmean and Cho/Cr) were combined with the PET parameter (mean target-to-background ratio), demonstrating an increase in diagnostic accuracy.
Conclusions: Simultaneous PET/MR imaging with FDG offers correlative and synergistic multiparametric assessment of glioma recurrence with increased accuracy and clinical utility.
© 2017 by American Journal of Neuroradiology.
Figures
Similar articles
-
Glioma Recurrence Versus Radiation Necrosis: Single-Session Multiparametric Approach Using Simultaneous O-(2-18F-Fluoroethyl)-L-Tyrosine PET/MRI.Clin Nucl Med. 2016 May;41(5):e228-36. doi: 10.1097/RLU.0000000000001152. Clin Nucl Med. 2016. PMID: 26859208
-
Potential for differentiation of glioma recurrence from radionecrosis using integrated 18F-fluoroethyl-L-tyrosine (FET) positron emission tomography/magnetic resonance imaging: A prospective evaluation.Neurol India. 2017 Mar-Apr;65(2):293-301. doi: 10.4103/neuroindia.NI_101_16. Neurol India. 2017. PMID: 28290392
-
Multiparametric Analysis Combining DSC-MR Perfusion and [18F]FET-PET is Superior to a Single Parameter Approach for Differentiation of Progressive Glioma from Radiation Necrosis.Clin Neuroradiol. 2024 Jun;34(2):351-360. doi: 10.1007/s00062-023-01372-1. Epub 2023 Dec 29. Clin Neuroradiol. 2024. PMID: 38157019
-
Diagnostic Accuracy of Amino Acid and FDG-PET in Differentiating Brain Metastasis Recurrence from Radionecrosis after Radiotherapy: A Systematic Review and Meta-Analysis.AJNR Am J Neuroradiol. 2018 Feb;39(2):280-288. doi: 10.3174/ajnr.A5472. Epub 2017 Dec 14. AJNR Am J Neuroradiol. 2018. PMID: 29242363 Free PMC article.
-
Diagnostic Performance of PET and Perfusion-Weighted Imaging in Differentiating Tumor Recurrence or Progression from Radiation Necrosis in Posttreatment Gliomas: A Review of Literature.AJNR Am J Neuroradiol. 2020 Sep;41(9):1550-1557. doi: 10.3174/ajnr.A6685. Epub 2020 Aug 27. AJNR Am J Neuroradiol. 2020. PMID: 32855194 Free PMC article. Review.
Cited by
-
Challenges and opportunities for advanced neuroimaging of glioblastoma.Br J Radiol. 2023 Jan 1;96(1141):20211232. doi: 10.1259/bjr.20211232. Epub 2022 Oct 14. Br J Radiol. 2023. PMID: 36062962 Free PMC article. Review.
-
Editorial: Global excellence in nuclear medicine: North America.Front Med (Lausanne). 2023 Oct 25;10:1300179. doi: 10.3389/fmed.2023.1300179. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37954553 Free PMC article. No abstract available.
-
Neuro-Oncology Practice Clinical Debate: FDG PET to differentiate glioblastoma recurrence from treatment-related changes.Neurooncol Pract. 2021 May 4;8(5):518-525. doi: 10.1093/nop/npab027. eCollection 2021 Oct. Neurooncol Pract. 2021. PMID: 34594566 Free PMC article. Review.
-
The Role of PET Imaging in the Differential Diagnosis between Radiation Necrosis and Recurrent Disease in Irradiated Adult-Type Diffuse Gliomas: A Systematic Review.Cancers (Basel). 2023 Jan 5;15(2):364. doi: 10.3390/cancers15020364. Cancers (Basel). 2023. PMID: 36672314 Free PMC article. Review.
-
Dual-energy spectral CT quantitative parameters for the differentiation of Glioma recurrence from treatment-related changes: a preliminary study.BMC Med Imaging. 2020 Jan 16;20(1):5. doi: 10.1186/s12880-019-0406-5. BMC Med Imaging. 2020. PMID: 31948400 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical