

Efficacy and safety of percutaneous ultrasound guided radiofrequency ablation for treating cervical metastatic lymph nodes from papillary thyroid carcinoma
- PMID: 28342000
- PMCID: PMC11819101
- DOI: 10.1007/s00432-017-2386-6
Efficacy and safety of percutaneous ultrasound guided radiofrequency ablation for treating cervical metastatic lymph nodes from papillary thyroid carcinoma
Abstract
Purpose: The aim of this study was to assess the effectiveness and safety of ultrasound guided percutaneous radiofrequency ablation (RFA) of cervical metastatic lymph nodes (LNs) from papillary thyroid carcinoma.
Methods: 54 metastatic LNs confirmed by percutaneous biopsy in 33 patients with previous total thyroidectomy and radioiodine therapy were enrolled in this retrospective study. US and contrast-enhanced ultrasound (CEUS) examinations were performed before ablation. Follow-up consisted of conventional US, CEUS, thyroglobulin (Tg) level at 1, 3, 6, and 12 months and every 6 months thereafter. In 3 months after ablation, US-guided core needle biopsy (CNB) was performed in the center, at the edge of the ablation area to exclude recurrence.
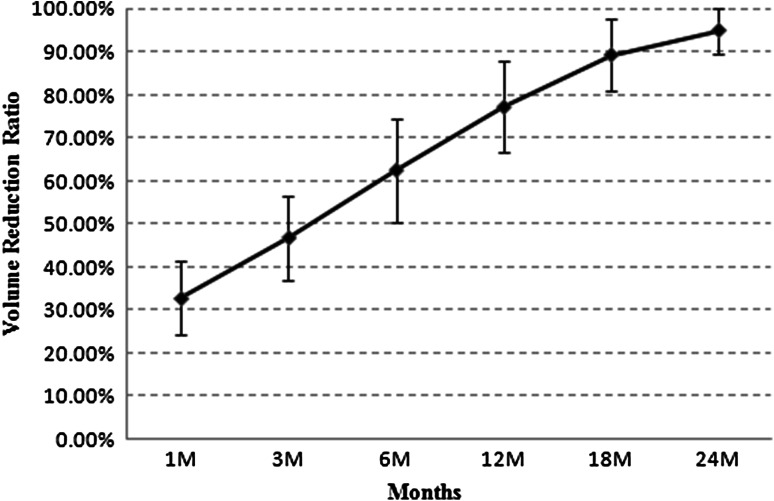
Results: Technical success was obtained in all 54 lymph nodes (100%) without immediate or later major complications occurred. With a mean follow-up of 21 ± 4 months (range 12-24 months), there were no evidence of recurrence at ablated sites. After RFA, 33 metastatic LNs completely disappeared (33/54, 61.1%) and 21 metastatic lymph nodes remained as small scarlike lesions (21/54, 38.9%) at the last follow-up visit. The mean volume reduction ratio (VRR) was 32.7 ± 8.6% (range 21.2-59.3%), 46.8 ± 9.7% (range 33.6-68.1%), 62.5 ± 12.1% (range 42.5-95.4%), 77.1 ± 10.6% (range 54.3-100.0%), 89.2 ± 8.3% (range 68.7-100.0%) and 94.9 ± 5.3% (range 78.2-100.0%) at 1, 3, 6, 12, 18 and 24 months after RFA respectively. Significant differences in the VRR were found between every two follow-up visits (P < 0.001). At the last follow-up visit, the mean serum Tg level decreased from 10.2 ± 5.1 ng/ml (range 0.8-16.2 ng/ml) to 1.1 ± 0.8 ng/ml (range 0.2-3.1 ng/ml) (P < 0.001).
Conclusions: Ultrasound guided percutaneous RFA for cervical metastatic LNs from papillary thyroid carcinoma is a feasible, effective and safe therapy. This procedure shows a nonsurgical therapeutic option that can eradicate the lesions with a very low complication rate.
Keywords: Metastatic lymph node; Papillary thyroid carcinoma; Radiofrequency ablation (RFA); Ultrasound.
Conflict of interest statement
All authors of this manuscript declare that they have no conflict of interest.
Figures

Comment in
-
Image-guided ablations in patients with thyroid tumors.J Cancer Res Clin Oncol. 2017 Dec;143(12):2637-2639. doi: 10.1007/s00432-017-2503-6. Epub 2017 Sep 2. J Cancer Res Clin Oncol. 2017. PMID: 28866839 Free PMC article. No abstract available.
Similar articles
-
Ultrasound-guided Radiofrequency Ablation for Cervical Lymph Nodes Metastasis from Papillary Thyroid Carcinoma.Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2018 Feb 28;40(1):67-71. doi: 10.3881/j.issn.1000-503X.2018.01.010. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2018. PMID: 29532783 English.
-
Ultrasound-Guided Radiofrequency Ablation versus Reoperation for Level VI Lymph Nodes Recurrence After Thyroidectomy.Acad Radiol. 2025 Sep;32(9):5082-5090. doi: 10.1016/j.acra.2025.05.060. Epub 2025 Jun 19. Acad Radiol. 2025. PMID: 40541550
-
Ultrasound‑guided Percutaneous Radiofrequency and Microwave Ablation for Cervical Lymph Node Metastasis from Papillary Thyroid Carcinoma: A Systematic Review and Meta‑analysis of Clinical Efficacy and Safety.Acad Radiol. 2025 May;32(5):2533-2544. doi: 10.1016/j.acra.2024.12.064. Epub 2025 Jan 11. Acad Radiol. 2025. PMID: 39800601
-
Ultrasonography-guided percutaneous radiofrequency ablation for cervical lymph node metastasis from thyroid carcinoma.J Cancer Res Ther. 2014 Nov;10 Suppl:C144-9. doi: 10.4103/0973-1482.145844. J Cancer Res Ther. 2014. PMID: 25450273
-
Therapeutic outcomes and safety of radiofrequency ablation for primary papillary thyroid carcinoma: A game-changing meta-analysis.Radiother Oncol. 2025 Apr;205:110706. doi: 10.1016/j.radonc.2025.110706. Epub 2025 Jan 23. Radiother Oncol. 2025. PMID: 39862924
Cited by
-
Value of contrast-enhanced ultrasonography in radiofrequency ablation of secondary hyperparathyroidism.Ren Fail. 2021 Dec;43(1):445-451. doi: 10.1080/0886022X.2021.1889601. Ren Fail. 2021. PMID: 33663332 Free PMC article.
-
Efficacy of ultrasound-guided core needle biopsy in cervical lymphadenopathy: A retrospective study of 6,695 cases.Eur Radiol. 2018 May;28(5):1809-1817. doi: 10.1007/s00330-017-5116-1. Epub 2017 Nov 29. Eur Radiol. 2018. PMID: 29188372
-
Preliminary report of microwave ablation for the primary papillary thyroid microcarcinoma: a large-cohort of 185 patients feasibility study.Endocrine. 2019 Apr;64(1):109-117. doi: 10.1007/s12020-019-01868-2. Epub 2019 Feb 15. Endocrine. 2019. PMID: 30771153
-
Thermal Ablation for Papillary Thyroid Carcinoma.JAMA Otolaryngol Head Neck Surg. 2024 Nov 7;151(1):9-17. doi: 10.1001/jamaoto.2024.3229. Online ahead of print. JAMA Otolaryngol Head Neck Surg. 2024. PMID: 39509126
-
Value of radiofrequency ablation for treating locally recurrent thyroid cancer: a systematic review and meta-analysis for 2-year follow-up.Endocrine. 2024 Sep;85(3):1066-1074. doi: 10.1007/s12020-023-03660-9. Epub 2024 May 27. Endocrine. 2024. PMID: 38801598
References
-
- Baek JH, Kim YS, Lee D, Huh JY, Lee JH (2010) Benign predominantly solid thyroid nodules: prospective study of efficacy of sonographically guided radiofrequency ablation versus control condition. AJR Am J Roentgenol 194(4):1137–1142. doi:10.2214/AJR.09.3372 - PubMed
-
- Baek JH, Kim YS, Sung JY, Choi H, Lee JH (2011) Locoregional control of metastatic well-differentiated thyroid cancer by ultrasound guided radiofrequency ablation. Am J Roentgenol 197(2):W331–W336. doi:10.2214/AJR.10.5345 - PubMed
-
- Burman KD (2012) Treatment of recurrent or persistent cervical node metastases in differentiated thyroid cancer: deceptively simple options. J Clin Endocrinol Metab 97(8):2623–2625. doi:10.1210/jc.2012-2480 - PubMed
-
- DeGroot LJ, Kaplan EL, McCormick M, Straus FH (1990) Natural history, treatment and course of papillary thyroid carcinoma. J Clin Endocrinol Metab 71(2):414–424. doi:10.1210/jcem-71-2-414 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
