

Real-time fMRI neurofeedback in adolescents with attention deficit hyperactivity disorder
- PMID: 28342214
- PMCID: PMC5434828
- DOI: 10.1002/hbm.23584
Real-time fMRI neurofeedback in adolescents with attention deficit hyperactivity disorder
Abstract
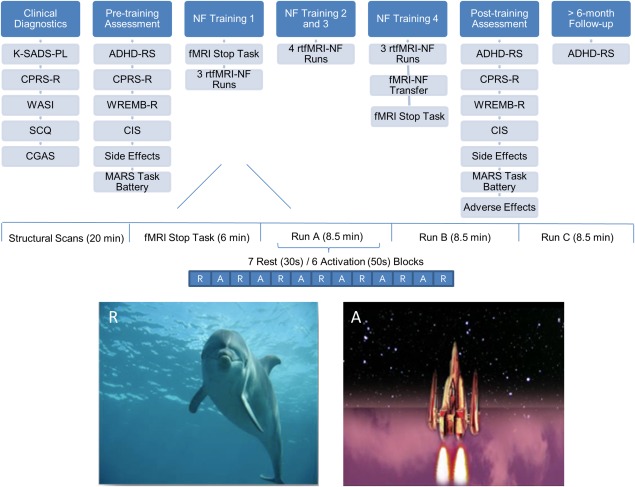
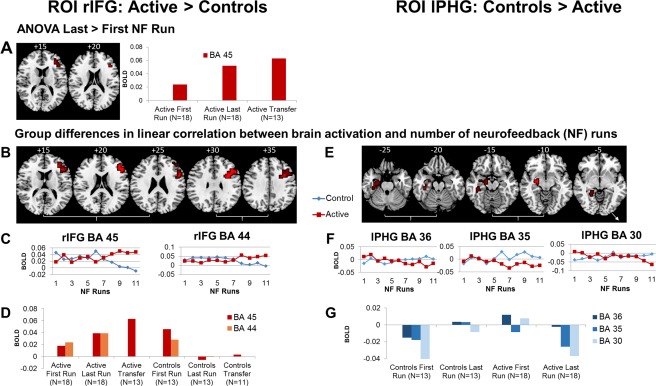
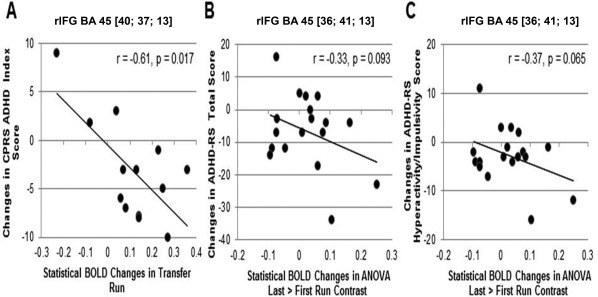
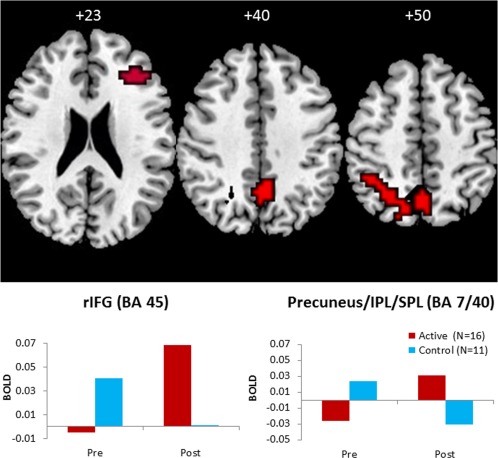
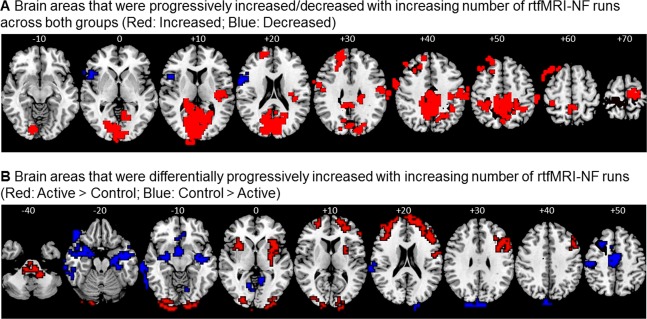
Attention Deficit Hyperactivity Disorder (ADHD) is associated with poor self-control, underpinned by inferior fronto-striatal deficits. Real-time functional magnetic resonance neurofeedback (rtfMRI-NF) allows participants to gain self-control over dysregulated brain regions. Despite evidence for beneficial effects of electrophysiological-NF on ADHD symptoms, no study has applied the spatially superior rtfMRI-NF neurotherapy to ADHD. A randomized controlled trial tested the efficacy of rtfMRI-NF of right inferior prefrontal cortex (rIFG), a key region that is compromised in ADHD and upregulated with psychostimulants, on improvement of ADHD symptoms, cognition, and inhibitory fMRI activation. To control for region-specificity, an active control group received rtfMRI-NF of the left parahippocampal gyrus (lPHG). Thirty-one ADHD boys were randomly allocated and had to learn to upregulate their target brain region in an average of 11 rtfMRI-NF runs over 2 weeks. Feedback was provided through a video-clip of a rocket that had to be moved up into space. A transfer session without feedback tested learning retention as a proximal measure of transfer to everyday life. Both NF groups showed significant linear activation increases with increasing number of runs in their respective target regions and significant reduction in ADHD symptoms after neurotherapy and at 11-month follow-up. Only the group targeting rIFG, however, showed a transfer effect, which correlated with ADHD symptom reductions, improved at trend level in sustained attention, and showed increased IFG activation during an inhibitory fMRI task. This proof-of-concept study demonstrates for the first time feasibility, safety, and shorter- and longer-term efficacy of rtfMRI-NF of rIFG in adolescents with ADHD. Hum Brain Mapp 38:3190-3209, 2017. © 2017 The Authors Human Brain Mapping Published by Wiley Periodicals, Inc.
Keywords: ADHD; fMRI; fMRI-neurofeedback; real-time fMRI neurofeedback; stop task.
© 2017 The Authors Human Brain Mapping Published by Wiley Periodicals, Inc.
Figures
References
-
- Arns M, Kenemans JL (2014): Neurofeedback in ADHD and insomnia: Vigilance stabilization through sleep spindles and circadian networks. Neurosci Biobehav Rev 44:183–194. - PubMed
-
- Arns M, de Ridder S, Strehl U, Breteler M, Coenen A (2009): Efficacy of neurofeedback treatment in ADHD: The effects on inattention, impulsivity and hyperactivity: A meta‐analysis. Clin EEG Neurosci 40:180–189. - PubMed
-
- Baumeister S, Wolf I, Holz N, Boecker‐Schlier R, Adamo N, Holtmann M, Ruf M, Banaschewski T, Hohmann S, Brandeis D (2016): Neurofeedback training effects on inhibitory brain activation in ADHD: A matter of learning? Neuroscience. doi: 10.1016/j.neuroscience.2016.09.025. [Epub ahead of print] - DOI - PubMed
-
- Bird HR, Shaffer D, Fisher P, Gould MS, Staghezza B, Chen JY, Hoven C (1993): The Columbia‐impairment‐scale (cis) ‐ pilot findings on a measure of global impairment for children and adolescents. Int J Methods Psychiatric Res 3:167–176.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
