

Hemoadsorption by CytoSorb in septic patients: a case series
- PMID: 28343448
- PMCID: PMC5366999
- DOI: 10.1186/s13054-017-1662-9
Hemoadsorption by CytoSorb in septic patients: a case series
Abstract
Background: Septic shock, defined as life-threatening organ dysfunction caused by a dysregulated host response to infection, is a highly lethal condition that causes substantial morbidity and mortality among critically ill patients. One of the hallmarks of sepsis is the excessive release of cytokines and other inflammatory mediators causing refractory hypotension, tissue damage, metabolic acidosis and ultimately multiple organ failure. In this context, cytokine reduction by hemoadsorption represents a new concept for blood purification, developed to attenuate the overwhelming systemic levels of pro-inflammatory and anti-inflammatory mediators released in the early phase of sepsis.
Methods: In the present case series, we evaluated the impact of a new hemoadsorption device (CytoSorb) used as adjunctive therapy, on hemodynamics and clinically relevant outcome parameters in 26 critically ill patients with septic shock and in need of renal replacement therapy.
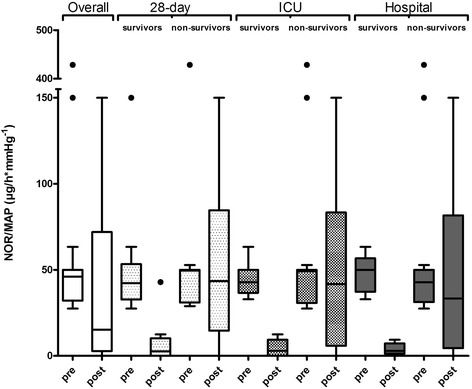
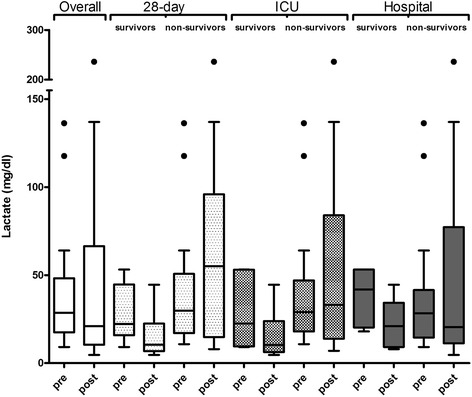
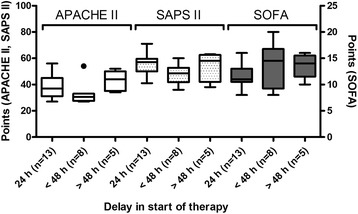
Results: We found that treatment of these patients with septic shock was associated with hemodynamic stabilization and a reduction in blood lactate levels. Actual mortality in the overall patient population was lower than mortality predicted by acute physiology and chronic health evaluation II (APACHE II). These effects seem to be more pronounced in patients in whom therapy started within 24 h of sepsis diagnosis, whereas a delay in the start of therapy was associated with a poor response to therapy in terms of reduction of catecholamine demand and survival. Moreover, from our patient population, medical patients seemed to benefit more than post-surgical patients in terms of survival. Treatment using the CytoSorb device was safe and well-tolerated with no device-related adverse events during or after the treatment sessions.
Conclusion: Hemoadsorption using CytoSorb resulted in rapid hemodynamic stabilization and increased survival, particularly in patients in whom therapy was started early. Given the positive clinical experience of this case series, randomized controlled trials are urgently needed to define the potential benefits of this new treatment option.
Keywords: Catecholamines; CytoSorb; Cytokine storm; Cytokines; Hemoadsorption; Hemodynamics; Hemoperfusion; Inflammation; Sepsis; Septic shock.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
