

Three-Dimensional Echocardiography: Current Status and Real-Life Applications
- PMID: 28344414
- PMCID: PMC5364152
- DOI: 10.6515/acs20160818a
Three-Dimensional Echocardiography: Current Status and Real-Life Applications
Abstract
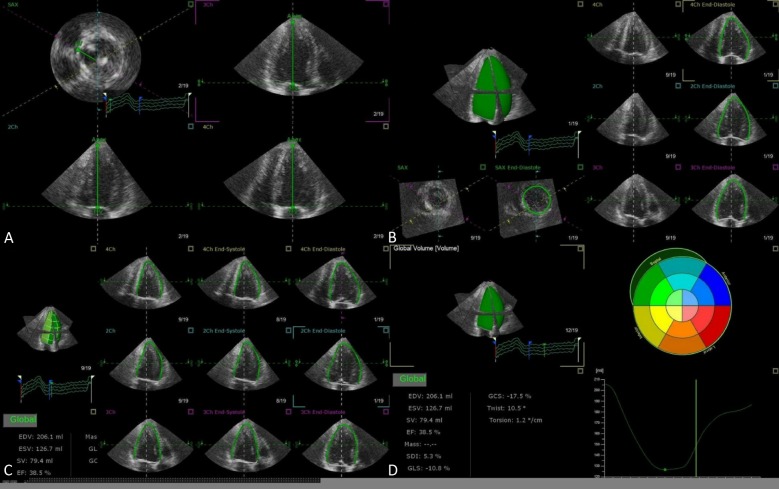
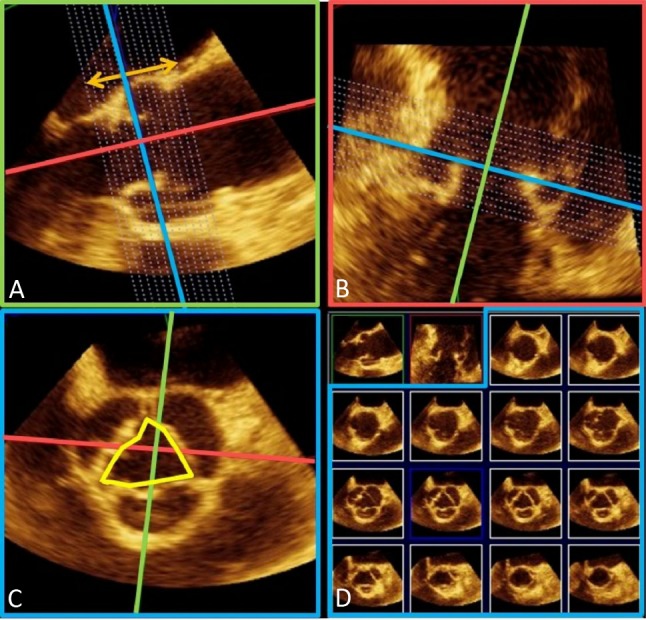
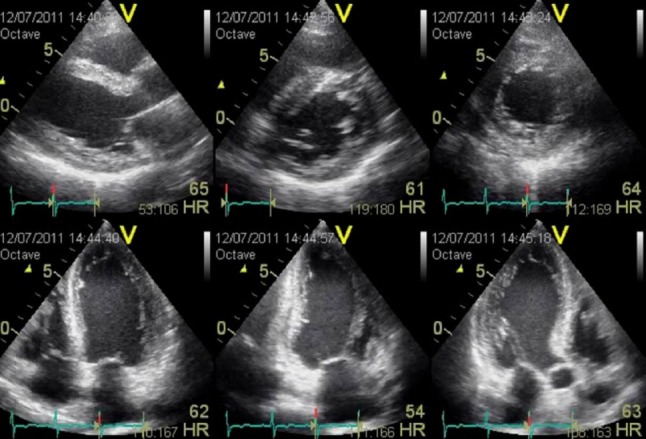
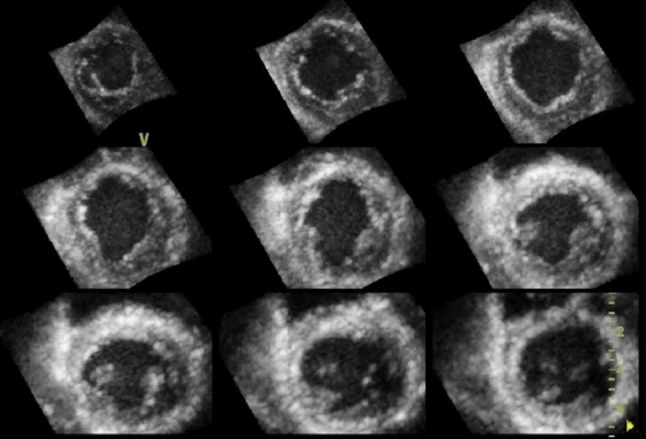
The use of cardiac ultrasound is fundamental to the understanding of normal heart function and crucial to pathophysiological diagnosis. The growing availability of 3D echocardiography (3DE) over the last decade has allowed its applications to expand from establishing reference values for chamber size and elucidating ventricular mechanics, to assessing valvular disease severity and playing pivotal roles in interventional procedures. Several important advantages of 3DE include eliminating geometric assumptions, quantifying complex geometric shape volumes, viewing structures from any perspective, assessing lesion in simultaneous multiplanes or multislice mode, all of which are not possible with traditional 2D echocardiography (2DE). Real-time 3DE has been shown to be simple, accurate, reproducible, and versatile, and generally has superior outcome prognosis compared to the 2DE.
Keywords: 3D echocardiography; Chamber mechanics; Valvular lesions.
Figures

References
-
- von Ramm OT, Smith SW. Real time volumetric ultrasound imaging system. J Digital Imaging. 1990;3:261–266. - PubMed
-
- Lang RM, Mor-Avi V, Dent JM, Kramer CM. Three-dimensional echocardiography: is it ready for everyday clinical use? JACC Cardiovasc Imaging. 2009;2:114–117. - PubMed
-
- Mor-Avi V, Sugeng L, Lang RM. Real-time 3-dimensional echocardiography: an integral component of the routine echocardiographic examination in adult patients? Circulation. 2009;119:314–329. - PubMed
-
- Lang RM, Badano LP, Tsang W, et al. American Society of Echocardiography; European Association of Echocardiography. EAE/ASE recommendations for image acquisition and display using three-dimensional echocardiography. JASE. 2012;25:3–46. - PubMed
-
- Jenkins C, Bricknell K, Hanekom L, Marwick TH. Reproducibility and accuracy of echocardiographic measurements of left ventricular parameters using real-time three-dimensional echocardiography. J Am Coll Cardiol. 2004;44:878–886. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources