

Missed diagnosis of stroke in the emergency department: a cross-sectional analysis of a large population-based sample
- PMID: 28344918
- PMCID: PMC5361750
- DOI: 10.1515/dx-2013-0038
Missed diagnosis of stroke in the emergency department: a cross-sectional analysis of a large population-based sample
Abstract
Background: Some cerebrovascular events are not diagnosed promptly, potentially resulting in death or disability from missed treatments. We sought to estimate the frequency of missed stroke and examine associations with patient, emergency department (ED), and hospital characteristics.
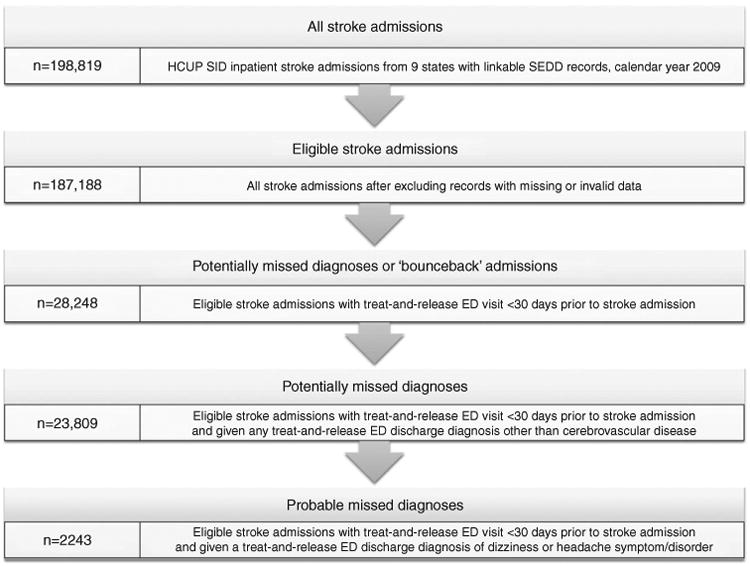
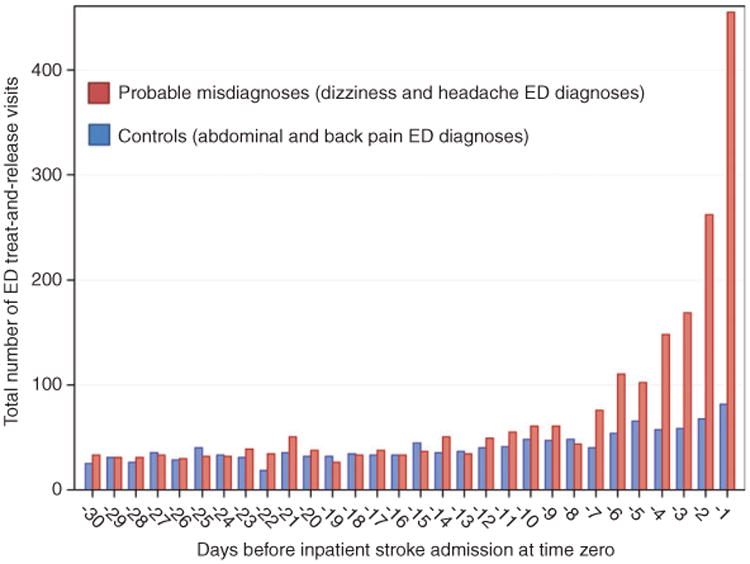
Methods: Cross-sectional analysis using linked inpatient discharge and ED visit records from the 2009 Healthcare Cost and Utilization Project State Inpatient Databases and 2008-2009 State ED Databases across nine US states. We identified adult patients admitted for stroke with a treat-and-release ED visit in the prior 30 days, considering those given a non-cerebrovascular diagnosis as probable (benign headache or dizziness diagnosis) or potential (any other diagnosis) missed strokes.
Results: There were 23,809 potential and 2243 probable missed strokes representing 12.7% and 1.2% of stroke admissions, respectively. Missed hemorrhages (n = 406) were linked to headache while missed ischemic strokes (n = 1435) and transient ischemic attacks (n = 402) were linked to headache or dizziness. Odds of a probable misdiagnosis were lower among men (OR 0.75), older individuals (18-44 years [base]; 45-64:OR 0.43; 65-74:OR 0.28; ≥ 75:OR 0.19), and Medicare (OR 0.66) or Medicaid (OR 0.70) recipients compared to privately insured patients. Odds were higher among Blacks (OR 1.18), Asian/Pacific Islanders (OR 1.29), and Hispanics (OR 1.30). Odds were higher in non-teaching hospitals (OR 1.45) and low-volume hospitals (OR 1.57).
Conclusions: We estimate 15,000-165,000 misdiagnosed cerebrovascular events annually in US EDs, disproportionately presenting with headache or dizziness. Physicians evaluating these symptoms should be particularly attuned to the possibility of stroke in younger, female, and non-White patients.
Keywords: cerebrovascular disorders; diagnostic errors; dizziness; emergency medical services; headache; vertigo.
Conflict of interest statement
Conflict of interest statement: Authors' conflict of interest disclosure: The authors stated that there are no conflicts of interest regarding the publication of this article. Research funding played no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the report for publication.
Figures
References
-
- Saber Tehrani AS, Lee H, Mathews SC, Shore A, Makary MA, Pronovost PJ, et al. 25-Year summary of US malpractice claims for diagnostic errors 1986-2010: an analysis from the National Practitioner Data Bank. BMJ Qual Saf. 2013;22:672–80. - PubMed
-
- Schiff GD, Hasan O, Kim S, Abrams R, Cosby K, Lambert BL, et al. Arch Intern Med. 2009;169:1881–7. - PubMed
-
- Kachalia A, Gandhi TK, Puopolo AL, Yoon C, Thomas EJ, Griffey R, et al. Missed and delayed diagnoses in the emergency department: a study of closed malpractice claims from 4 liability insurers. Ann Emerg Med. 2007;49:196–205. - PubMed
-
- Dubois RW, Brook RH. Preventable deaths: who, how often, and why? Ann Intern Med. 1988;109:582–9. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources