

CXCL12 Promotes Stem Cell Recruitment and Uterine Repair after Injury in Asherman's Syndrome
- PMID: 28345002
- PMCID: PMC5363300
- DOI: 10.1016/j.omtm.2017.01.001
CXCL12 Promotes Stem Cell Recruitment and Uterine Repair after Injury in Asherman's Syndrome
Abstract
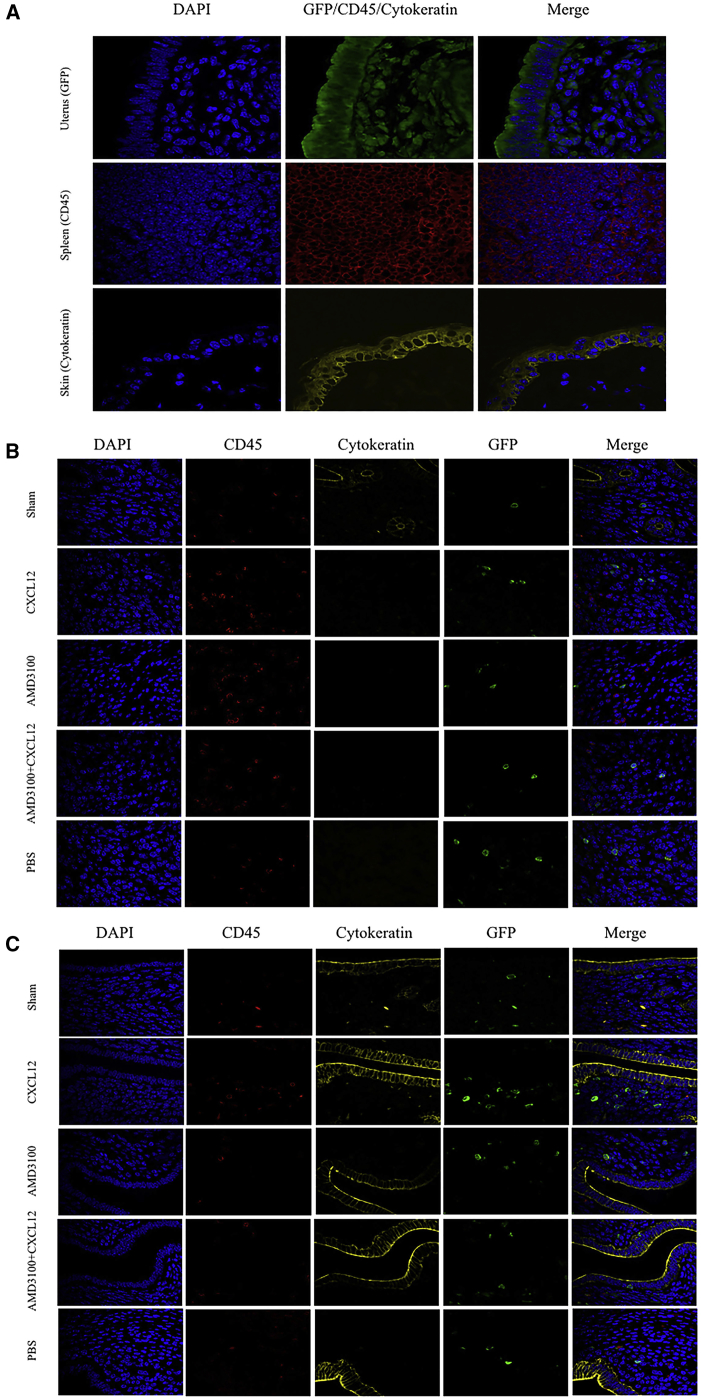
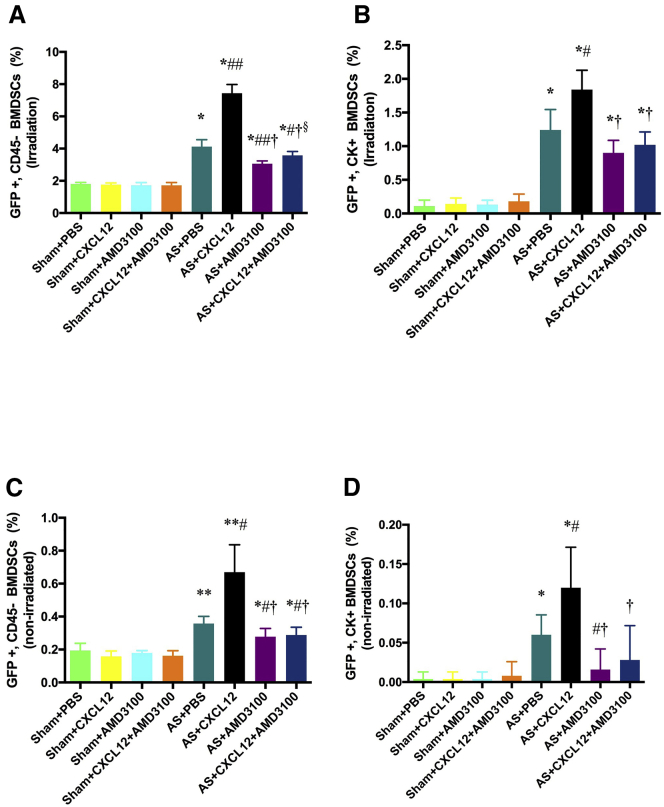
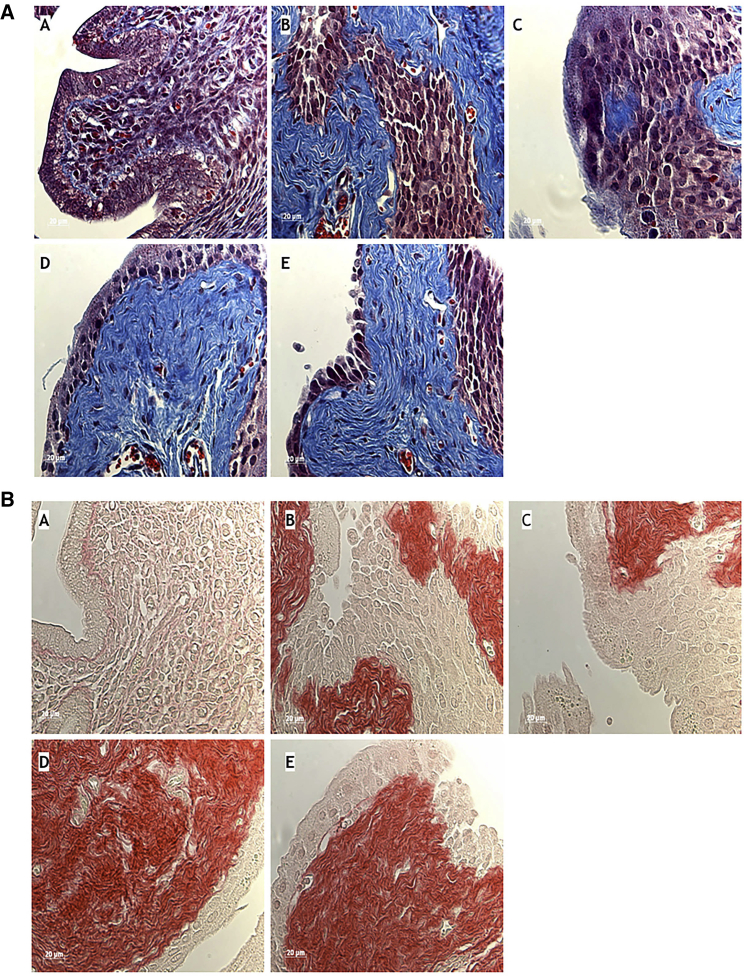
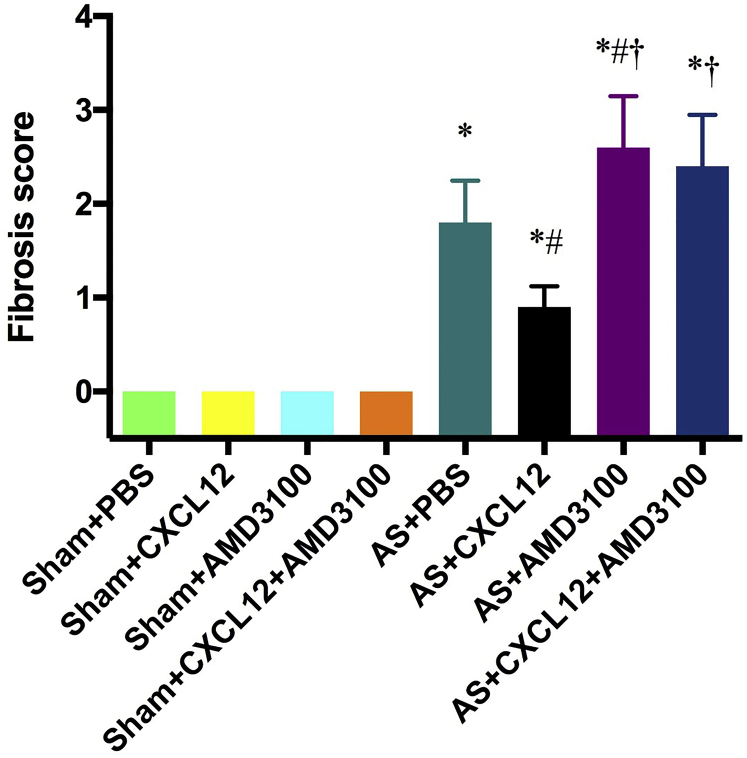
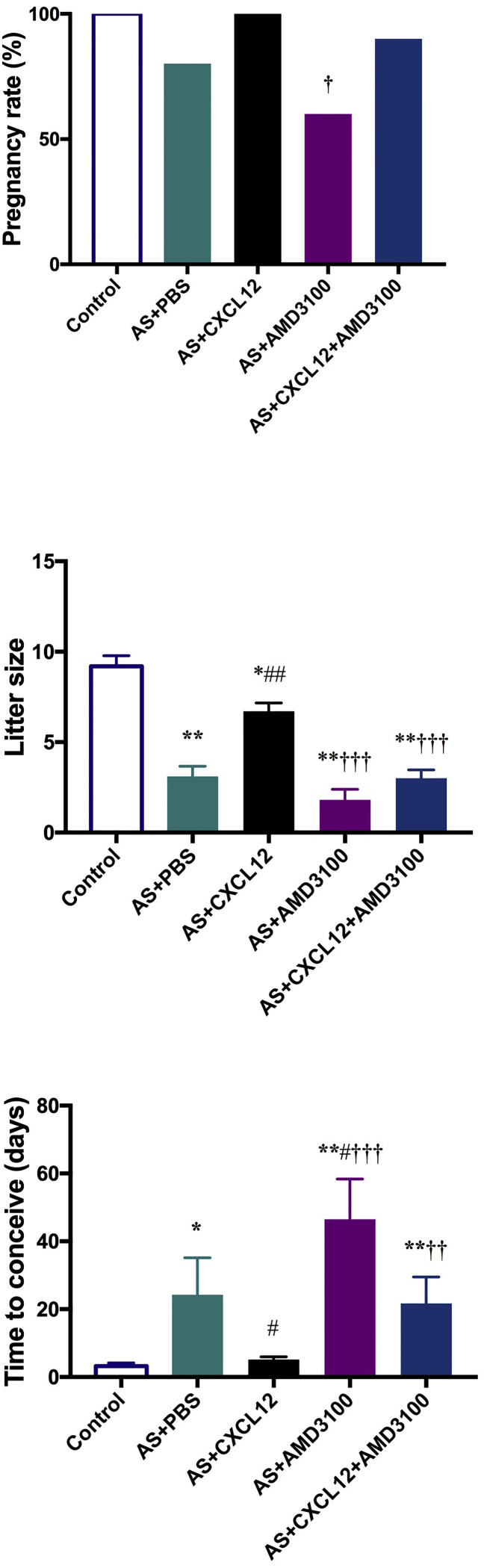
Asherman's syndrome is an acquired condition of uterine fibrosis and adhesions in response to injury that adversely affects fertility and pregnancy. We have previously demonstrated that bone marrow-derived mesenchymal stem cells (BMDSCs) contribute to uterine repair after injury and that stem cells supplementation improves fertility. Here, we demonstrate that CXCL12 is the chemokine that mediates stem cell engraftment and functional improvement using a murine model of Asherman's syndrome. After uterine injury, we demonstrate that CXCL12 augmentation increased BMDSC engraftment and that the CXCL12 receptor (CXCR4) antagonist, ADM3100, blocked stem cell recruitment. CXCL12 reduced, whereas ADM3100 increased fibrosis. CXCL12 treatment led to improved fertility and litter size, whereas ADM3100 treatment reduced fertility and litter size. ADM3100 prevented optimal spontaneous uterine repair mediated by endogenous CXCL12 production, reducing pregnancies after injury in the absence of supplemental CXCL12 administration; however, ADM3100 treatment could be partially rescued by CXCL12 augmentation. CXCL12 or other CXCR4 receptor agonists may be useful in the treatment of infertility or adverse pregnancy outcomes in Asherman's syndrome and other related uterine disorders.
Keywords: AMD3100; Asherman’s syndrome; CXCL12; CXCR4; cell therapy; fertility; intrauterine adhesions; stem cells; uterus.
Figures
Similar articles
-
Bone Marrow-Derived Stem Cell (BMDSC) transplantation improves fertility in a murine model of Asherman's syndrome.PLoS One. 2014 May 12;9(5):e96662. doi: 10.1371/journal.pone.0096662. eCollection 2014. PLoS One. 2014. PMID: 24819371 Free PMC article.
-
A matched cohort study comparing the outcome of intrauterine adhesiolysis for Asherman's syndrome after uterine artery embolization or surgical trauma.J Minim Invasive Gynecol. 2014 Nov-Dec;21(6):1022-8. doi: 10.1016/j.jmig.2014.04.015. Epub 2014 May 16. J Minim Invasive Gynecol. 2014. PMID: 24842805
-
Hysteroscopic adhesiolysis for patients with Asherman's syndrome: menstrual and fertility outcomes.Reprod Med Biol. 2013 May 5;12(4):159-166. doi: 10.1007/s12522-013-0149-x. eCollection 2013 Oct. Reprod Med Biol. 2013. PMID: 29662367 Free PMC article.
-
Endometrial Regeneration in Asherman's Syndrome: Clinical and Translational evidence of Stem Cell Therapies.Curr Stem Cell Res Ther. 2019;14(6):454-459. doi: 10.2174/1574888X14666190213100528. Curr Stem Cell Res Ther. 2019. PMID: 30760192 Review.
-
Making More Womb: Clinical Perspectives Supporting the Development and Utilization of Mesenchymal Stem Cell Therapy for Endometrial Regeneration and Infertility.J Pers Med. 2021 Dec 14;11(12):1364. doi: 10.3390/jpm11121364. J Pers Med. 2021. PMID: 34945836 Free PMC article. Review.
Cited by
-
miR-466 and NUS1 Regulate the AKT/Nuclear Factor kappa B (NFκB) Signaling Pathway in Intrauterine Adhesions in a Rat Model.Med Sci Monit. 2019 Jun 2;25:4094-4103. doi: 10.12659/MSM.914202. Med Sci Monit. 2019. PMID: 31154456 Free PMC article.
-
The application of tissue engineering strategies for uterine regeneration.Mater Today Bio. 2025 Feb 18;31:101594. doi: 10.1016/j.mtbio.2025.101594. eCollection 2025 Apr. Mater Today Bio. 2025. PMID: 40070871 Free PMC article. Review.
-
Stem Cell-Based Therapy for Asherman Syndrome: Promises and Challenges.Cell Transplant. 2021 Jan-Dec;30:9636897211020734. doi: 10.1177/09636897211020734. Cell Transplant. 2021. PMID: 34105392 Free PMC article. Review.
-
Bone marrow-derived progenitor cells contribute to remodeling of the postpartum uterus.Stem Cells. 2021 Nov;39(11):1489-1505. doi: 10.1002/stem.3431. Epub 2021 Aug 6. Stem Cells. 2021. PMID: 34224633 Free PMC article.
-
Chemokine Therapy in Cats With Experimental Renal Fibrosis and in a Kidney Disease Pilot Study.Front Vet Sci. 2021 Mar 4;8:646087. doi: 10.3389/fvets.2021.646087. eCollection 2021. Front Vet Sci. 2021. PMID: 33748219 Free PMC article.
References
-
- Kodaman P.H., Arici A. Intra-uterine adhesions and fertility outcome: how to optimize success? Curr. Opin. Obstet. Gynecol. 2007;19:207–214. - PubMed
-
- Buttram V.C., Jr., Turati G. Uterine synechiae: variations in severity and some conditions which may be conducive to severe adhesions. Int. J. Fertil. 1977;22:98–103. - PubMed
-
- Klein S.M., García C.R. Asherman’s syndrome: a critique and current review. Fertil. Steril. 1973;24:722–735. - PubMed
-
- Yu D., Wong Y.M., Cheong Y., Xia E., Li T.C. Asherman syndrome—one century later. Fertil. Steril. 2008;89:759–779. - PubMed
-
- Tuuli M.G., Shanks A., Bernhard L., Odibo A.O., Macones G.A., Cahill A. Uterine synechiae and pregnancy complications. Obstet. Gynecol. 2012;119:810–814. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
