

Peroneal perforator pedicle propeller flap for lower leg soft tissue defect reconstruction: Clinical applications and treatment of venous congestion
- PMID: 28345420
- PMCID: PMC5536429
- DOI: 10.1177/0300060516687229
Peroneal perforator pedicle propeller flap for lower leg soft tissue defect reconstruction: Clinical applications and treatment of venous congestion
Abstract
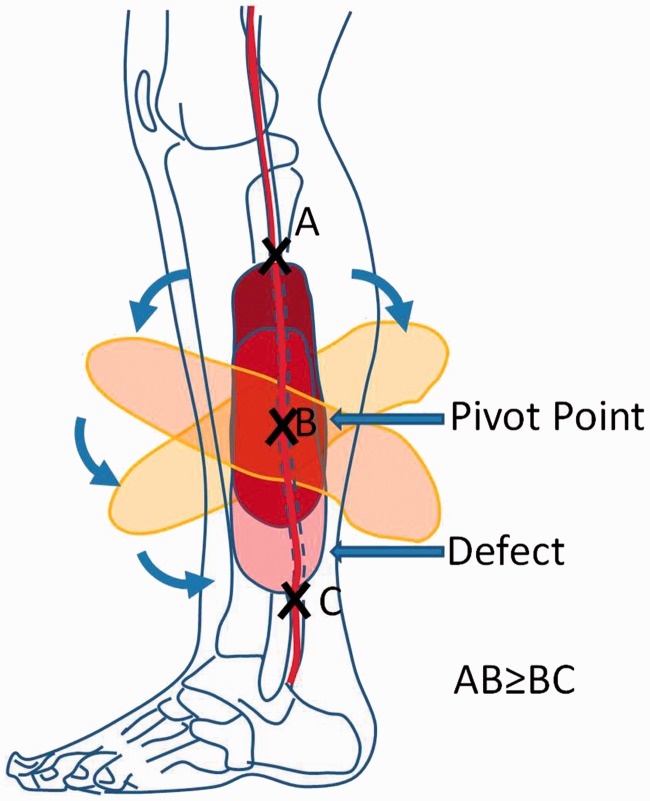
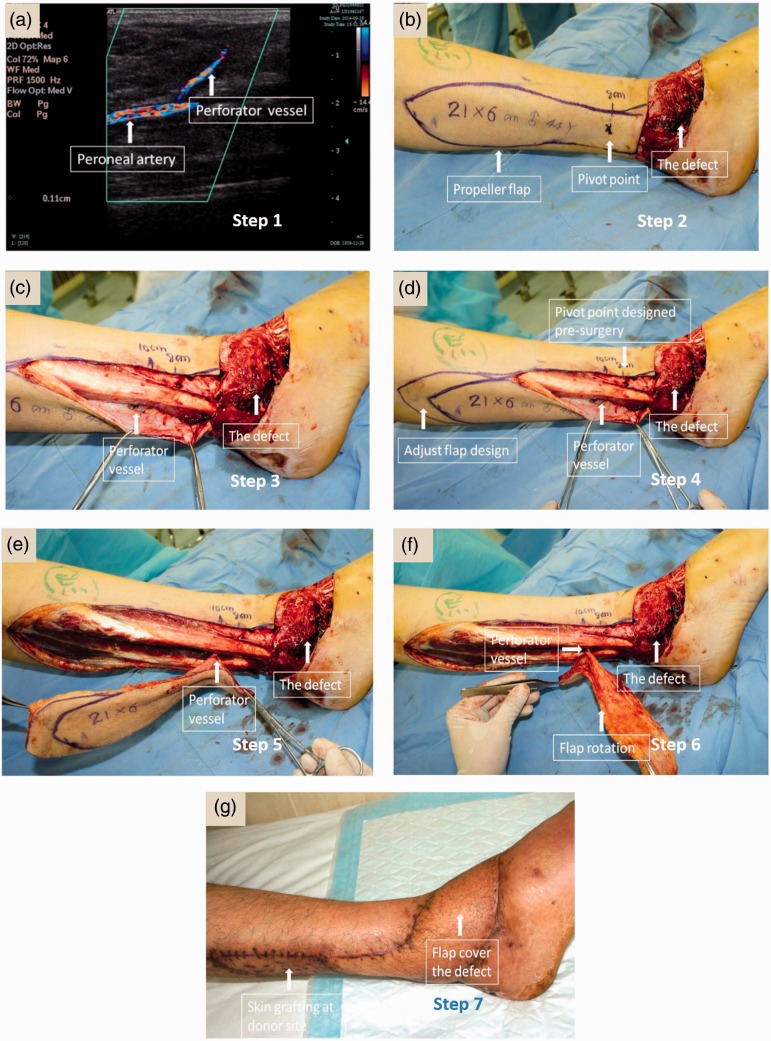
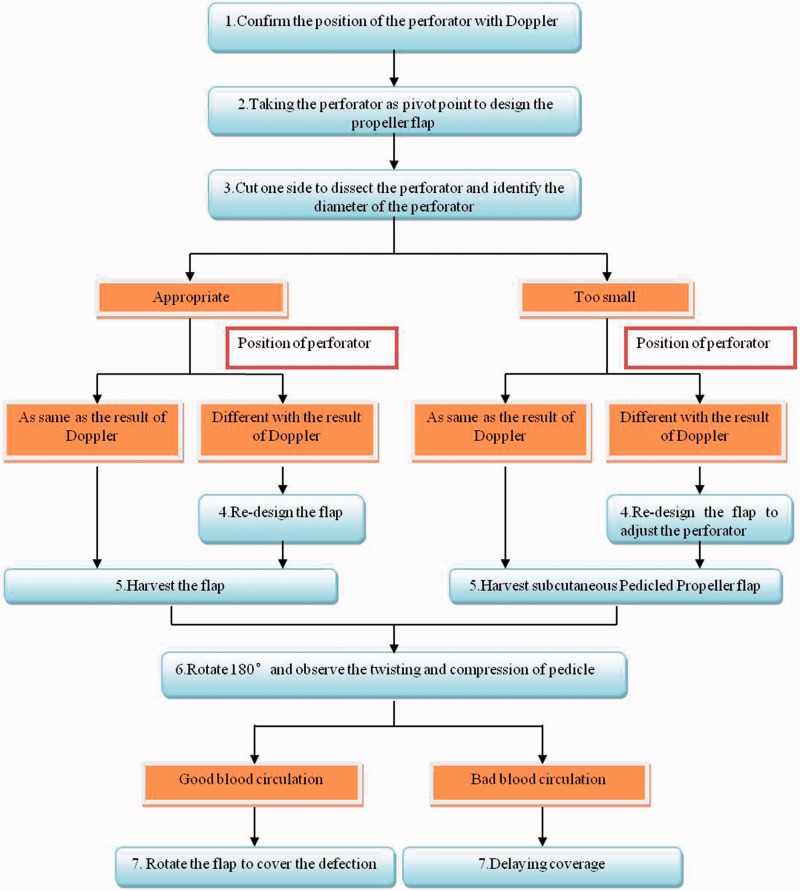
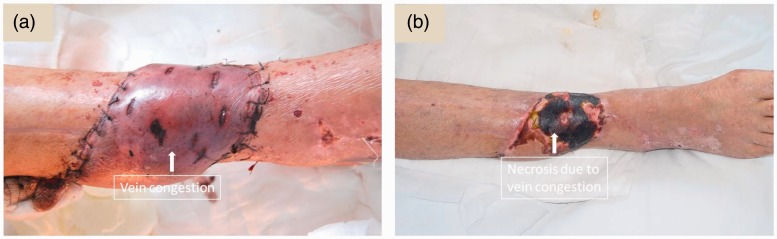
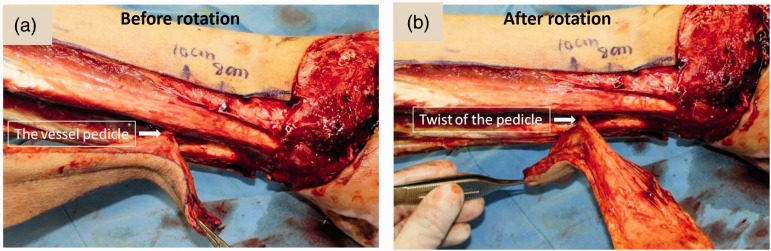
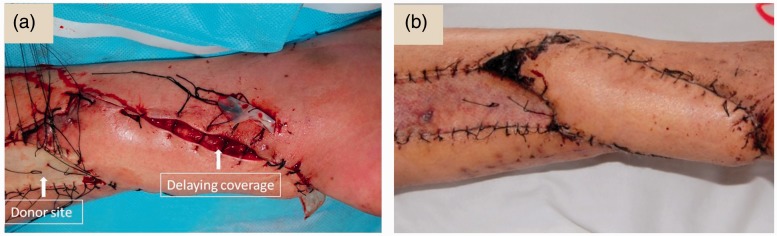
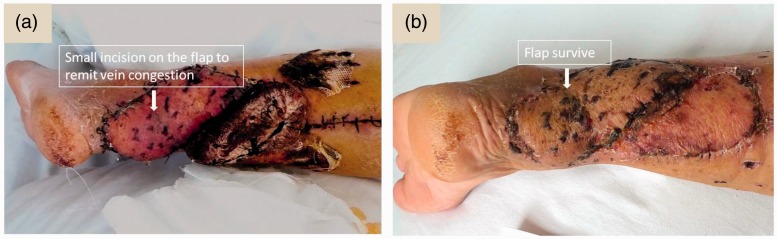
Objective To describe the characteristics of the perforator vessel in the peroneal artery of the lower leg and to explore the use of perforator pedicle propeller flaps to repair soft tissue defects in the lower leg, heel and foot. Methods This retrospective study enrolled patients with soft tissue defects of the distal lower leg, heel and foot who underwent surgery using peroneal perforator-based propeller flaps. The peroneal artery perforators were identified preoperatively by colour duplex Doppler ultrasound. The flap was designed based on the preoperatively-identified perforator location, with the posterior border of the fibula employed as an axis, and the perforator vessel as the pivot point of rotation. Patients were followed-up to determine the outcomes. Results The study analysed 36 patients (mean age, 39.7 years). The majority of the soft tissue defects were on the heel (20; 55.6%). The donor-site of the flap was closed in 11 patients by direct suturing and skin grafting was undertaken in 25 patients. Postoperative complications included venous congestion (nine patients), which was managed with delayed wound coverage and bleeding therapy. All wounds were eventually cured and the flaps were cosmetically acceptable. Conclusions The peroneal perforator pedicle propeller flap is an appropriate choice to repair soft tissue defects of the distal limbs.
Keywords: Perforator-based propeller flaps; congestion; peroneal artery; soft tissue reconstruction.
Figures

Similar articles
-
[Application of perforator propeller flap sequential transfer technique in repair of soft tissue defect of distal lower extremity].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2022 Apr 15;36(4):451-455. doi: 10.7507/1002-1892.202111047. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2022. PMID: 35426285 Free PMC article. Chinese.
-
Perforator Propeller Flap "Relay" for Distal Lower Extremity Soft Tissue Reconstruction.J Foot Ankle Surg. 2020 Sep-Oct;59(5):1128-1132. doi: 10.1053/j.jfas.2020.05.012. Epub 2020 May 31. J Foot Ankle Surg. 2020. PMID: 32703651
-
[Anterior tibial artery perforator propeller flap relay peroneal artery terminal perforator propeller flap for foot and ankle defect].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2020 Jan 15;34(1):87-91. doi: 10.7507/1002-1892.201904095. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2020. PMID: 31939241 Free PMC article. Chinese.
-
Freestyle Local Island Pedicle Flap in Lower Leg Reconstruction.Clin Plast Surg. 2021 Apr;48(2):193-200. doi: 10.1016/j.cps.2020.12.004. Epub 2021 Jan 29. Clin Plast Surg. 2021. PMID: 33674041 Review.
-
Extensive Defect Reconstruction Using Multiple Perforator Propeller Flaps in a Jigsaw Puzzle Approach.Plast Reconstr Surg. 2024 Dec 1;154(6):1233e-1243e. doi: 10.1097/PRS.0000000000011286. Epub 2024 Jan 8. Plast Reconstr Surg. 2024. PMID: 38194621
Cited by
-
Use of Propeller Flap in the Coverage of Soft-Tissue Injury in the Lower Limb.Rev Bras Ortop (Sao Paulo). 2021 Apr;56(2):192-197. doi: 10.1055/s-0040-1714223. Epub 2020 Sep 25. Rev Bras Ortop (Sao Paulo). 2021. PMID: 33935314 Free PMC article.
-
Efficacy of combining a medial superior malleolar perforator flap from the posterior tibial artery with a vacuum-assisted closure dressing for skin and soft tissue defects of the Achilles tendon area.Am J Transl Res. 2024 Apr 15;16(4):1209-1218. doi: 10.62347/LSIM3562. eCollection 2024. Am J Transl Res. 2024. PMID: 38715817 Free PMC article.
-
Double-pedicle propeller flap for reconstruction of the foot and ankle: anatomical study and clinical applications.J Int Med Res. 2019 Oct;47(10):4775-4786. doi: 10.1177/0300060519865625. Epub 2019 Aug 5. J Int Med Res. 2019. PMID: 31378112 Free PMC article.
-
[Clinical application of digital technology in repairing of heel wound with peroneal artery perforator propeller flap].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2020 Mar 15;34(3):367-372. doi: 10.7507/1002-1892.201908079. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2020. PMID: 32174085 Free PMC article. Chinese.
-
Pedicled perforator flaps for mid-tibial soft tissue reconstruction in medically compromised patients.JPRAS Open. 2020 Feb 25;24:47-55. doi: 10.1016/j.jpra.2020.02.002. eCollection 2020 Jun. JPRAS Open. 2020. PMID: 32346592 Free PMC article.
References
-
- Chang SM, Hou CL, Xu DC. An overview of skin flap surgery in the mainland china: 20 years’ achievements (1981 to 2000). J Reconstr Microsurg 2009; 25: 361–367. - PubMed
-
- Chen YL, Zheng BG, Zhu JM, et al. Microsurgical anatomy of the lateral skin flap of the leg. Ann Plast Surg 1985; 15: 313–318. - PubMed
-
- Chesnier I, Bali D, Casanova D, et al. Flaps in lower limb reconstruction: a 10-year retrospective review of 157 pedicled flaps. Ann Chir Plast Esthet 2012; 57: 328–335. [in French, English Abstract]. - PubMed
-
- Jakubietz RG, Jakubietz DF, Gruenert JG, et al. Reconstruction of soft tissue defects of the Achilles tendon with rotation flaps, pedicled propeller flaps and free perforator flaps. Microsurgery 2010; 30: 608–613. - PubMed
-
- Lo CH, Leung M, Baillieu C, et al. Trauma centre experience: flap reconstruction of traumatic lower limb injuries. ANZ J Surg 2007; 77: 690–694. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
