

The Economic Burden of Opioid Abuse: Updated Findings
- PMID: 28345440
- PMCID: PMC10398023
- DOI: 10.18553/jmcp.2017.16265
The Economic Burden of Opioid Abuse: Updated Findings
Abstract
Background: Opioid pain relievers can be highly effective in providing relief for patients suffering from pain. At the same time, prescription opioid abuse, dependence, overdose, and poisoning (hereinafter "abuse") have become a national public health concern. Opioid abuse is also costly: previous estimates of the annual excess costs of opioid abuse to payers range from approximately $10,000 to $20,000 per patient.
Objectives: To (a) provide a comprehensive, current estimate of the economic burden of opioid abuse to commercial payers and (b) explore the drivers of these excess costs of abuse.
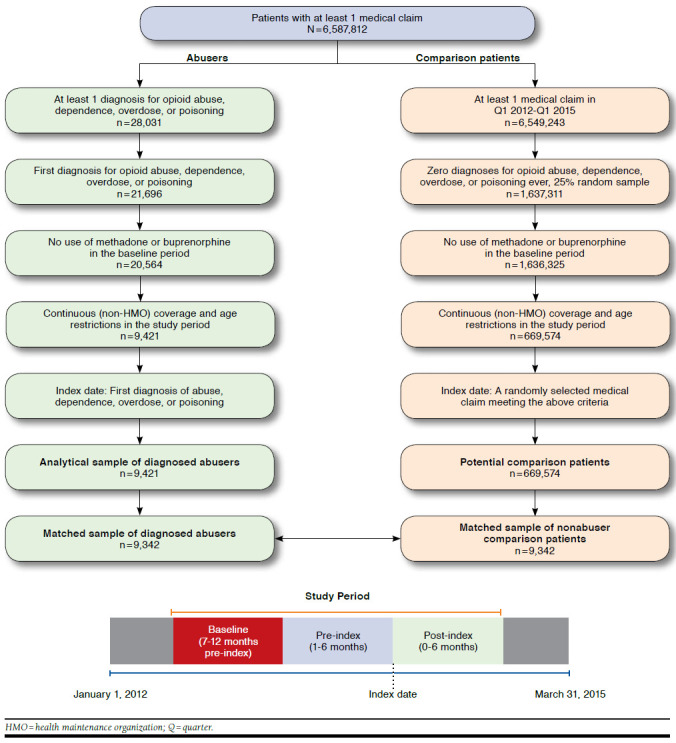
Methods: Administrative claims from beneficiaries covered by large self-insured companies throughout the United States were used to identify patients diagnosed with opioid abuse, dependence, and overdose/poisoning ("abuse") between 2012 and 2015. Sample selection criteria identified patients most likely to be misusing opioids. Abusers and nonabuser controls were matched using propensity scores. Excess health care costs were assessed over the 18-month study period. Drivers of excess costs were then evaluated by place of service and medical condition (identified as 3-digit ICD-9-CM groupings).
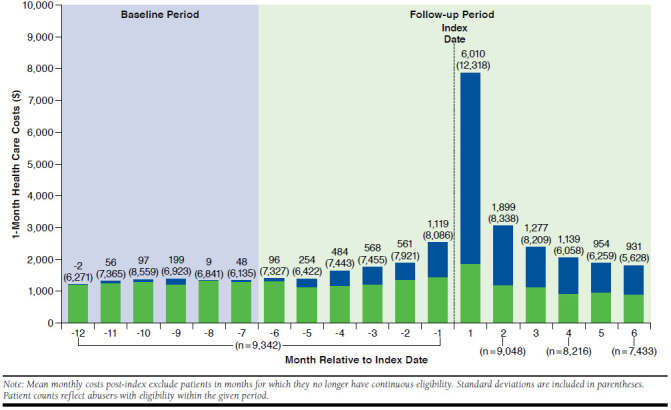
Results: 9,342 matched abuser/nonabuser pairs were analyzed. Relative to nonabusers, abusers had significantly higher annual health care resource utilization, leading to $14,810 in per-patient incremental annual health care costs. Excess costs began accumulating 5 months before the formal, incident diagnosis of abuse, driven by alcohol and nonopioid substance abuse. Major drivers of excess costs of abuse included opioid and other substance abuse disorders, mental health conditions, and painful conditions. Many patients had diagnoses for other substance abuse that predated their opioid abuse diagnoses.
Conclusions: Opioid abuse imposes a substantial economic burden on payers and often occurs in the context of other substance abuse. Poly-substance abuse often precedes the diagnosis of opioid abuse.
Disclosures: This study was funded by Purdue Pharma. Mayne is an employee of Purdue Pharma. Kirson, Scarpati, and Birnbaum are employees of Analysis Group, which received funding from Purdue Pharma to conduct this study. Enloe and Dincer were employees of Analysis Group at the time this research was conducted. Study concept and design were contributed by Kirson, Birnbaum, Mayne, and Scarpati, along with Enloe and Dincer. Enloe and Dincer took the lead in data collection, along with Birnbaum and assisted by Kirson and Scarpati. Data interpretation was performed by all the authors. The manuscript was written and revised by Kirson and Scarpati, along with Mayne and Birnbaum.
Conflict of interest statement
This study was funded by Purdue Pharma. Mayne is an employee of Purdue Pharma. Kirson, Scarpati, and Birnbaum are employees of Analysis Group, which received funding from Purdue Pharma to conduct this study. Enloe and Dincer were employees of Analysis Group at the time this research was conducted.
Study concept and design were contributed by Kirson, Birnbaum, Mayne, and Scarpati, along with Enloe and Dincer. Enloe and Dincer took the lead in data collection, along with Birnbaum and assisted by Kirson and Scarpati. Data interpretation was performed by all the authors. The manuscript was written and revised by Kirson and Scarpati, along with Mayne and Birnbaum.
Figures
References
-
- Simon LS. Relieving pain in America: a blueprint for transforming prevention, care, education, and research. J Pain Palliat Care Pharmacother. 2012;26(2):197-98.
-
- Gaskin DJ, Richard P.. The economic costs of pain in the United States. J Pain. 2012;13(8):715-24. - PubMed
-
- Carey TS, Garrett J, Jackman A, McLaughlin C, Fryer J, Smucker DR.. The outcomes and costs of care for acute low back pain among patients seen by primary care practitioners, chiropractors, and orthopedic surgeons. New Engl J Med. 1995;333(14):913-17. - PubMed
-
- Morley S, Eccleston C, Williams A.. Systematic review and meta-analysis of randomized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache. Pain. 1999;80(1):1-13. - PubMed
-
- Volkow ND. America’s addiction to opioids: heroin and prescription drug abuse. May 14, 2014. Available at: https://www.drugabuse.gov/about-nida/legislative-activities/testimony-to.... Accessed December 15, 2016.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
