

Economic Burden of Irritable Bowel Syndrome with Diarrhea: Retrospective Analysis of a U.S. Commercially Insured Population
- PMID: 28345443
- PMCID: PMC10398241
- DOI: 10.18553/jmcp.2016.16138
Economic Burden of Irritable Bowel Syndrome with Diarrhea: Retrospective Analysis of a U.S. Commercially Insured Population
Abstract
Background: The economic burden associated with irritable bowel syndrome with diarrhea (IBS-D) is not well understood.
Objectives: To (a) evaluate total annual all-cause, gastrointestinal (GI)-related, and symptom-related (i.e., IBS, diarrhea, abdominal pain) health care resource use and costs among IBS-D patients in a U.S. commercially insured population and (b) estimate incremental all-cause health care costs of IBS-D patients versus matched controls.
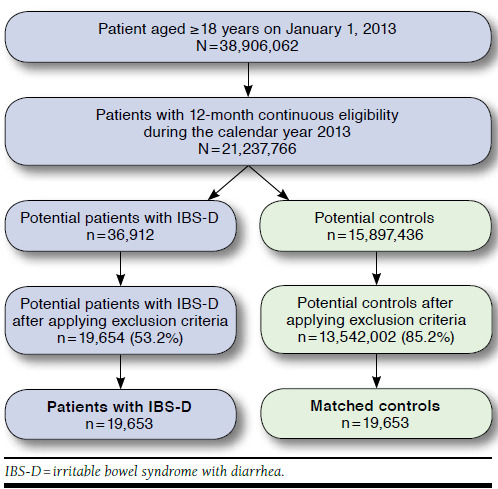
Methods: Patients aged ≥ 18 years with 12 months of continuous medical and pharmacy benefit eligibility in 2013 were identified from the Truven Health MarketScan research database. The study sample included patients with ≥ 1 medical claim with an International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis code in any position for IBS (ICD-9-CM 564.1x) and either (a) ≥ 2 claims for diarrhea (ICD-9-CM 787.91, 564.5x) on different service dates in 2013, or (b) ≥ 1 claim for diarrhea plus ≥ 1 claim for abdominal pain (ICD-9-CM 789.0x) on different service dates in 2013, or (c) ≥ 1 claim for diarrhea plus ≥ 1 pharmacy claim for a symptom-related prescription on different service dates in 2013. Controls included patients with no claims for IBS, diarrhea, abdominal pain, or symptom-related prescriptions in 2013. Controls were randomly selected and matched with IBS-D patients in a 1:1 ratio based on age (± 4 years), gender, geographic location, and health plan type. All-cause health care resource utilization included medical and pharmacy claims for health care services associated with any condition. Total health care costs were defined as the sum of health plan-paid and patient-paid direct health care costs from prescriptions and medical services, including inpatient, emergency department (ED), and physician office visits, and other outpatient services. A total cost approach was used to assess all-cause, GI-related, and symptom-related health care costs for IBS-D patients. An incremental cost approach via generalized linear models was used to assess the excess all-cause costs attributable to IBS-D after adjusting for demographics and general and GI comorbidities.
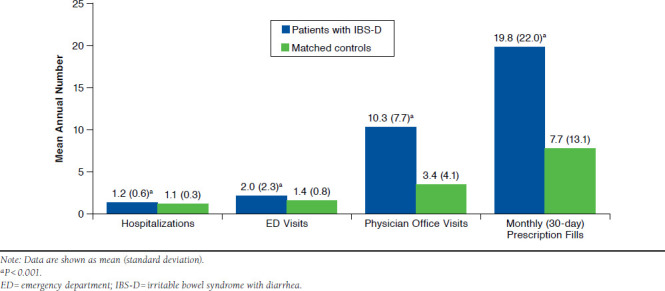
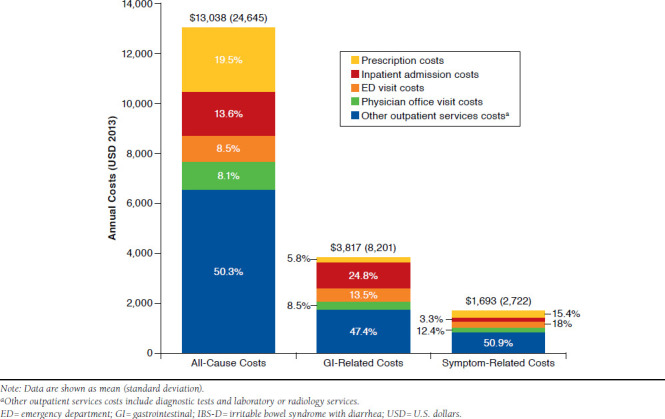
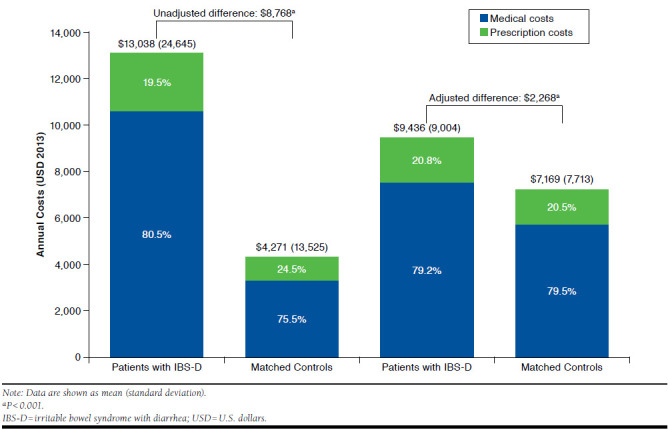
Results: Of 39,306 patients (n = 19,653 each for IBS-D and matched controls) included, mean (± SD) age was 47 (± 17) years and 76.5% were female. Compared with controls, IBS-D patients had a significantly higher mean annual number of hospitalizations, ED visits, office visits, and monthly (30-day) prescription fills. Mean annual all-cause health care costs for IBS-D patients were $13,038, with over half (58.4%) attributable to office visits and other outpatient services (e.g., diagnostic tests and laboratory or radiology services), and remaining costs attributable to prescriptions (19.5%), inpatient admissions (13.6%), and ED visits (8.5%). GI-related ($3,817) and symptom-related ($1,693) costs were also primarily driven by other outpatient service costs. After adjusting for demographics and comorbidities, incremental annual all-cause costs associated with IBS-D were $2,268 ($9,436 for IBS-D patients vs. $7,169 for matched controls; P < 0.001) per patient/year, of which 78% were from medical costs and 22% were from prescription costs.
Conclusions: IBS-D was associated with a substantial burden in direct costs in this population. Compared with matched controls, IBS-D patients had greater medical service use and incurred significantly more annual all-cause health care costs, even after controlling for demographics and comorbidities. Incremental costs associated with IBS-D were primarily attributable to increased use of medical services rather than pharmacy costs.
Disclosures: This study was funded by Allergan. The authors received no compensation related to the development of the manuscript. Buono and Andrae are employees of Allergan. Mathur is an employee of Axtria. Averitt was an employee of Axtria at the time this study was conducted. Data from this manuscript have previously been presented in poster format by Buono at the American College of Gastroenterology Annual Scientific Meeting; Honolulu, Hawaii; October 16-21, 2015. Mathur and Averitt were involved in conducting the study analyses. All authors were involved in the study design, interpretation of the data, and preparation of the manuscript. The authors take full responsibility for the scope, direction, and content of the manuscript and have approved the submitted manuscript.
Conflict of interest statement
This study was funded by Allergan. The authors received no compensation related to the development of the manuscript. Buono and Andrae are employees of Allergan. Mathur is an employee of Axtria. Averitt was an employee of Axtria at the time this study was conducted.
Data from this manuscript have previously been presented in poster format by Buono at the American College of Gastroenterology Annual Scientific Meeting; Honolulu, Hawaii; October 16-21, 2015.
Mathur and Averitt were involved in conducting the study analyses. All authors were involved in the study design, interpretation of the data, and preparation of the manuscript. The authors take full responsibility for the scope, direction, and content of the manuscript and have approved the submitted manuscript.
Figures
References
-
- Cash BD, Chey WD.. Irritable bowel syndrome - an evidence-based approach to diagnosis. Aliment Pharmacol Ther. 2004;19(12):1235-45. - PubMed
-
- Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC.. Functional bowel disorders. Gastroenterology. 2006;130(5):1480-91. - PubMed
-
- Hulisz D. The burden of illness of irritable bowel syndrome: current challenges and hope for the future. J Manag Care Pharm. 2004;10(4):299-309. Available at: http://www.jmcp.org/doi/abs/10.18553/jmcp.2004.10.4.299. - DOI - PMC - PubMed
-
- Saito YA, Schoenfeld P, Locke GR.. The epidemiology of irritable bowel syndrome in North America: a systematic review. Am J Gastroenterol. 2002;97(8):1910-15. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
