

Admission Glucose and In-hospital Mortality after Acute Myocardial Infarction in Patients with or without Diabetes: A Cross-sectional Study
- PMID: 28345539
- PMCID: PMC5381309
- DOI: 10.4103/0366-6999.202733
Admission Glucose and In-hospital Mortality after Acute Myocardial Infarction in Patients with or without Diabetes: A Cross-sectional Study
Abstract
Background: Hyperglycemia on admission has been found to elevate risk for mortality and adverse clinical events after acute myocardial infarction (AMI), but there are evidences that the relationship of blood glucose and mortality may differ between diabetic and nondiabetic patients. Prior studies in China have provided mixed results and are limited by statistical power. Here, we used data from a large, nationally representative sample of patients hospitalized with AMI in China in 2001, 2006, and 2011 to assess if admission glucose is of prognostic value in China and if this relationship differs depending on the presence or absence of diabetes.
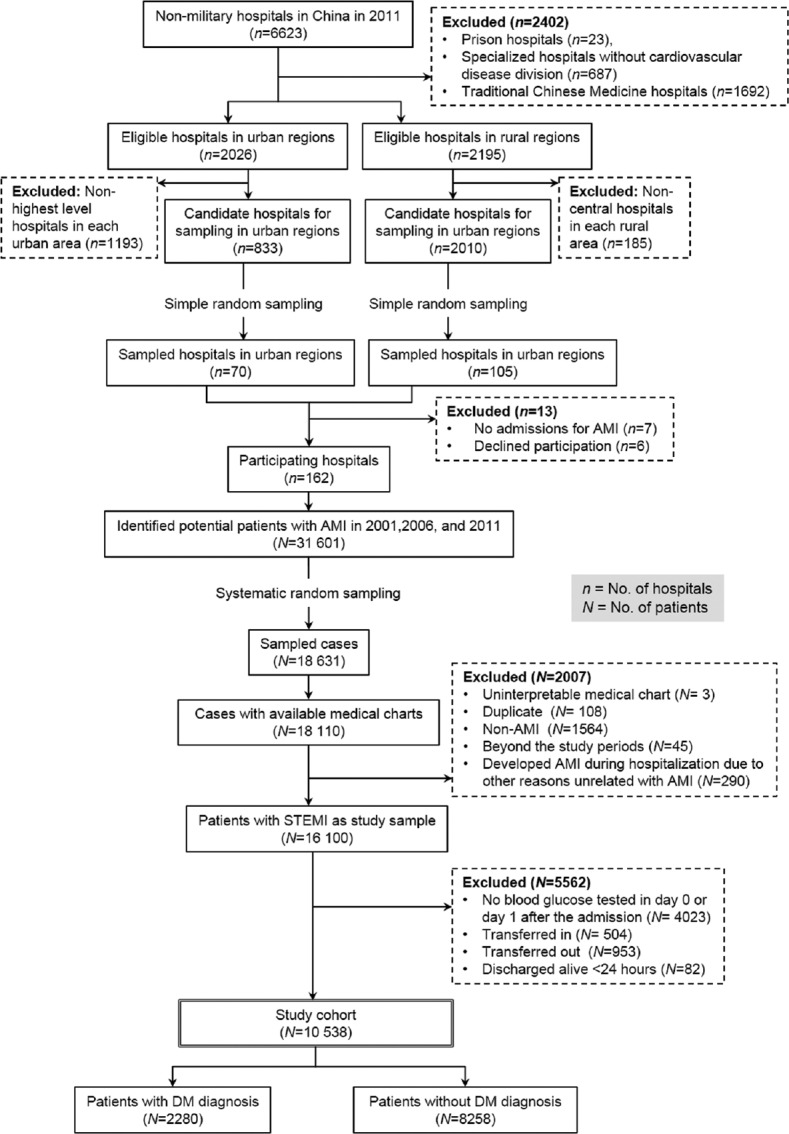
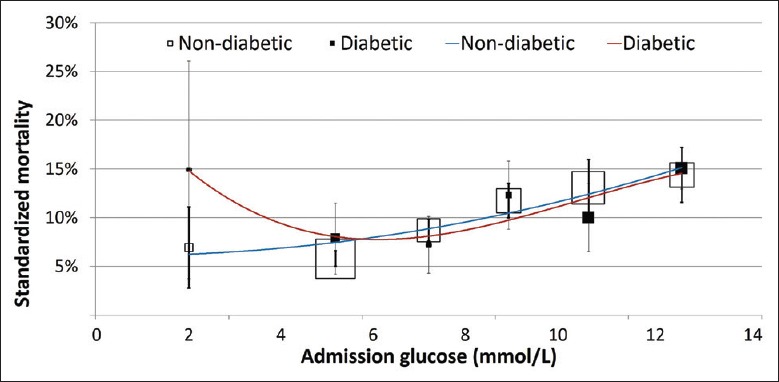
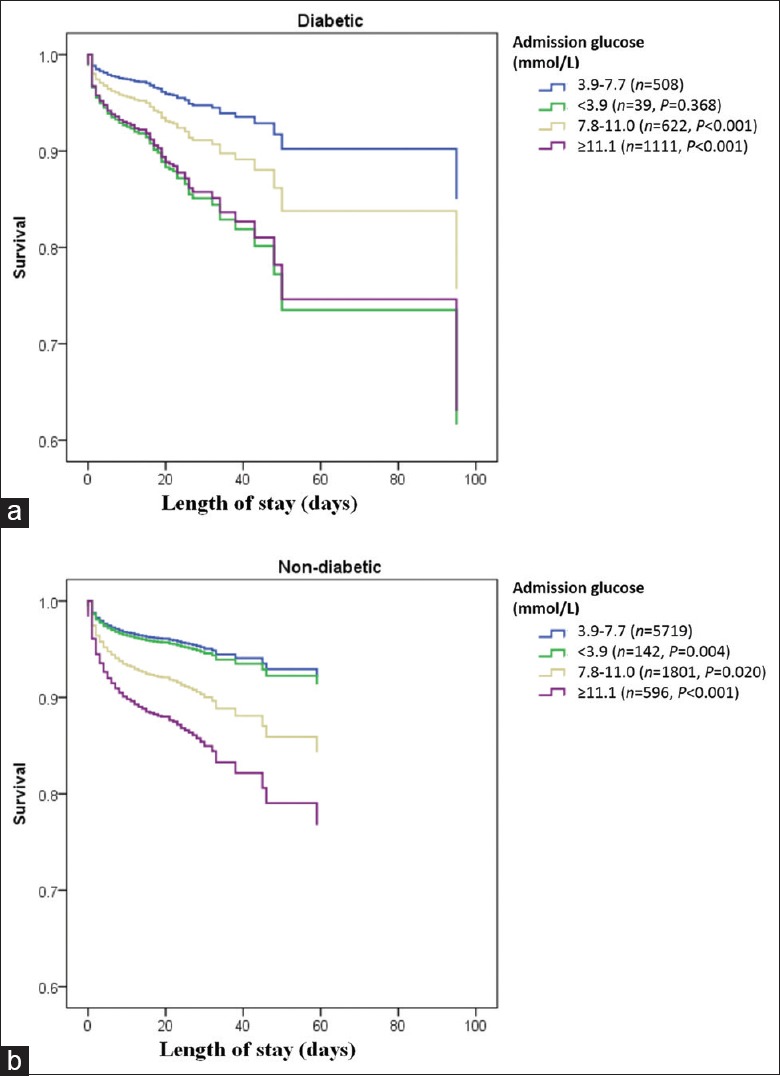
Methods: Using a nationally representative sample of patients with AMI in China in 2001, 2006, and 2011, we categorized patients according to their glucose levels at admission (Results: Compared to patients with euglycemia (5.8%), patients with moderate hyperglycemia (13.1%, odds ratio [OR] = 2.44, 95% confidence interval [CI, 2.08-2.86]), severe hyperglycemia (21.5%, OR = 4.42, 95% CI [3.78-5.18]), and hypoglycemia (13.8%, OR = 2.59, 95% CI [1.68-4.00]), all had higher crude in-hospital mortality after AMI regardless of the presence of recognized diabetes mellitus. After adjustment for patients' characteristics and clinical status, however, the relationship between admission glucose and in-hospital mortality was different for diabetic and nondiabetic patients (P for interaction = 0.045). Among diabetic patients, hypoglycemia (OR = 3.02, 95% CI [1.20-7.63]), moderate hyperglycemia (OR = 1.75, 95% CI [1.04-2.92]), and severe hyperglycemia (OR = 2.97, 95% CI [1.87-4.71]) remained associated with elevated risk for mortality, but among nondiabetic patients, only patients with moderate hyperglycemia (OR = 2.34, 95% CI [1.93-2.84]) and severe hyperglycemia (OR = 3.92, 95% CI [3.04-5.04]) were at elevated mortality risk and not hypoglycemia (OR = 1.12, 95% CI [0.60-2.08]). This relationship was consistent across different study years (P for interaction = 0.900).
Conclusions: The relationship between admission glucose and in-hospital mortality differs for diabetic and nondiabetic patients. Hypoglycemia was a bad prognostic marker among diabetic patients alone. The study results could be used to guide risk assessment among AMI patients using admission glucose.
Trial registration: www.clinicaltrials.gov, NCT01624883; https://clinicaltrials.gov/ct2/show/NCT01624883.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Capes SE, Hunt D, Malmberg K, Gerstein HC. Stress hyperglycaemia and increased risk of death after myocardial infarction in patients with and without diabetes: A systematic overview. Lancet. 2000;355:773–8. doi: 10.1016/S0140-6736(99)08415-9. - PubMed
-
- Kosiborod M, Rathore SS, Inzucchi SE, Masoudi FA, Wang Y, Havranek EP, et al. Admission glucose and mortality in elderly patients hospitalized with acute myocardial infarction: Implications for patients with and without recognized diabetes. Circulation. 2005;111:3078–86. doi: 10.1161/CIRCULATIONAHA.104.517839. - PubMed
-
- Wahab NN, Cowden EA, Pearce NJ, Gardner MJ, Merry H, Cox JL. ICONS Investigators. Is blood glucose an independent predictor of mortality in acute myocardial infarction in the thrombolytic era? J Am Coll Cardiol. 2002;40:1748–54. doi: 10.1016/S0735-1097(02)02483-X. - PubMed
-
- Kosiborod M, Inzucchi SE, Krumholz HM, Xiao L, Jones PG, Fiske S, et al. Glucometrics in patients hospitalized with acute myocardial infarction: Defining the optimal outcomes-based measure of risk. Circulation. 2008;117:1018–27. doi: 10.1161/CIRCULATIONAHA.107.740498. - PubMed
-
- Ishihara M, Kojima S, Sakamoto T, Kimura K, Kosuge M, Asada Y, et al. Comparison of blood glucose values on admission for acute myocardial infarction in patients with versus without diabetes mellitus. Am J Cardiol. 2009;104:769–74. doi: 10.1016/j.amjcard.2009.04.055. - PubMed
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
