

Insight into high myopia and the macula
- PMID: 28345561
- PMCID: PMC5381305
- DOI: 10.4103/ijo.IJO_863_16
Insight into high myopia and the macula
Abstract
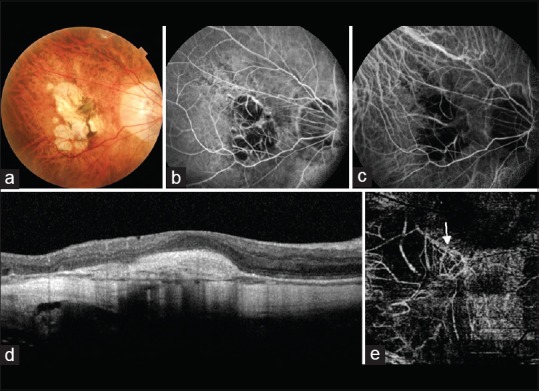
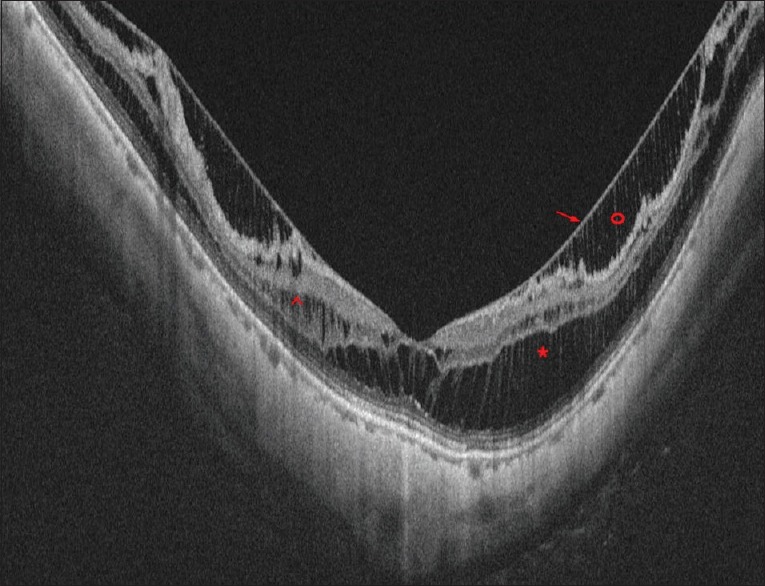
The incidence of myopia is constantly on the rise. Patients of high myopia and pathological myopia are young and can lose vision due to a number of degenerative changes occurring at the macula. With the emergence of new technologies such as swept-source optical coherence tomography (OCT) and OCT angiography, our understanding of macular pathology in myopia has improved significantly. New conditions such as myopic traction maculopathy have been defined. Early, noninvasive detection of myopic choroidal neovascularization and its differentiation from lacquer cracks is possible with a greater degree of certainty. We discuss the impact of these new exciting and promising technologies and management of macular pathology in myopia. Incorporation of OCT in the microscope has also improved macular surgery. New concepts such as fovea-sparing internal limiting membrane peeling have emerged. A review of literature and our experience in managing all these conditions are discussed.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Morgan IG, Ohno-Matsui K, Saw SM. Myopia. Lancet. 2012;379:1739–48. - PubMed
-
- Miller DG, Singerman LJ. Natural history of choroidal neovascularization in high myopia. Curr Opin Ophthalmol. 2001;12:222–4. - PubMed
-
- Hayashi K, Ohno-Matsui K, Shimada N, Moriyama M, Kojima A, Hayashi W, et al. Long-term pattern of progression of myopic maculopathy: A natural history study. Ophthalmology. 2010;117:1595–611. 1611.e1–4. - PubMed
-
- Curtin BJ, Karlin DB. Axial length measurements and fundus changes of the myopic eye. Am J Ophthalmol. 1971;71(1 Pt 1):42–53. - PubMed
-
- Wong TY, Ferreira A, Hughes R, Carter G, Mitchell P. Epidemiology and disease burden of pathologic myopia and myopic choroidal neovascularization: An evidence-based systematic review. Am J Ophthalmol. 2014;157:9–25.e12. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
