

Innovations in glaucoma surgery from Dr. Rajendra Prasad Centre for Ophthalmic Sciences
- PMID: 28345564
- PMCID: PMC5381287
- DOI: 10.4103/ijo.IJO_865_16
Innovations in glaucoma surgery from Dr. Rajendra Prasad Centre for Ophthalmic Sciences
Abstract
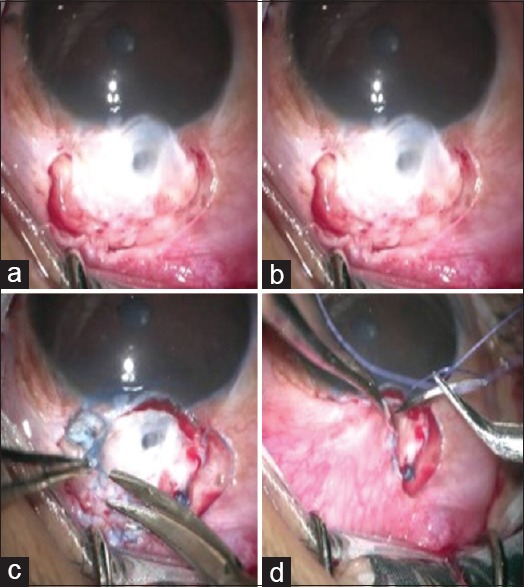
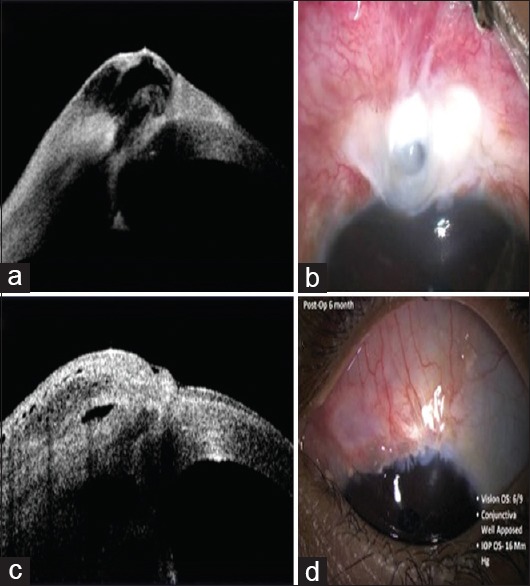
Trabeculectomy surgery is the current standard of care in glaucoma for achieving a low target intraocular pressure if medical therapy is not adequate. Augmentation of trabeculectomy with antimetabolites brought a revolutionary change in the long-term success rates of trabeculectomy, but along with it came a plethora of complications. There still is a big window for therapeutic innovations on this subject. The foremost target for these innovations is to modulate the wound healing response after glaucoma drainage surgery. Achieving the desired balance between long-term success of filtering blebs versus early failure due to scarring of blebs and hypotony due to dysfunctional filtering blebs poses a unique challenge to the ophthalmologists. Alternatives to trabeculectomy such as glaucoma drainage devices and minimally invasive glaucoma surgeries cannot solve the problem of glaucoma blindness in our country, mainly due to their unpredictable results and unfavorable cost-benefit ratio. In this article, we present a summary of our innovations in glaucoma surgery to advance patient care by making it more effective, safer, and economical.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Cairns JE. Trabeculectomy. Preliminary report of a new method. Am J Ophthalmol. 1968;66:673–9. - PubMed
-
- Landers J, Martin K, Sarkies N, Bourne R, Watson P. A twenty-year follow-up study of trabeculectomy: Risk factors and outcomes. Ophthalmology. 2012;119:694–702. - PubMed
-
- Higashide T, Ohkubo S, Sugimoto Y, Kiuchi Y, Sugiyama K. Persistent hypotony after trabeculectomy: Incidence and associated factors in the Collaborative Bleb-related Infection Incidence and Treatment Study. Jpn J Ophthalmol. 2016;60:309–18. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
