

Adding fast-acting insulin aspart to basal insulin significantly improved glycaemic control in patients with type 2 diabetes: A randomized, 18-week, open-label, phase 3 trial (onset 3)
- PMID: 28345792
- PMCID: PMC5637905
- DOI: 10.1111/dom.12955
Adding fast-acting insulin aspart to basal insulin significantly improved glycaemic control in patients with type 2 diabetes: A randomized, 18-week, open-label, phase 3 trial (onset 3)
Abstract
Aim: To confirm glycaemic control superiority of mealtime fast-acting insulin aspart (faster aspart) in a basal-bolus (BB) regimen vs basal-only insulin.
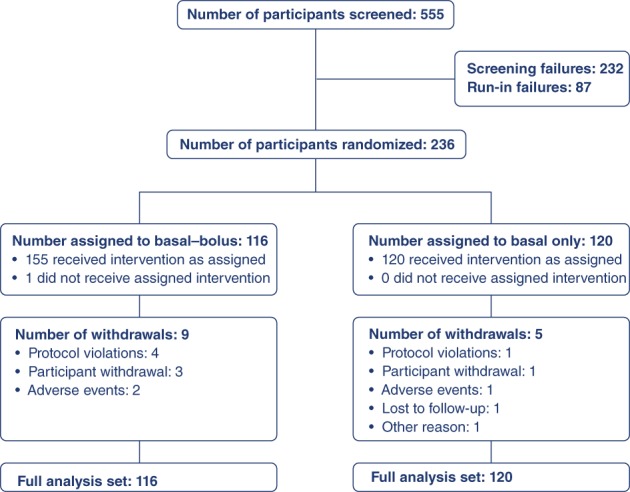
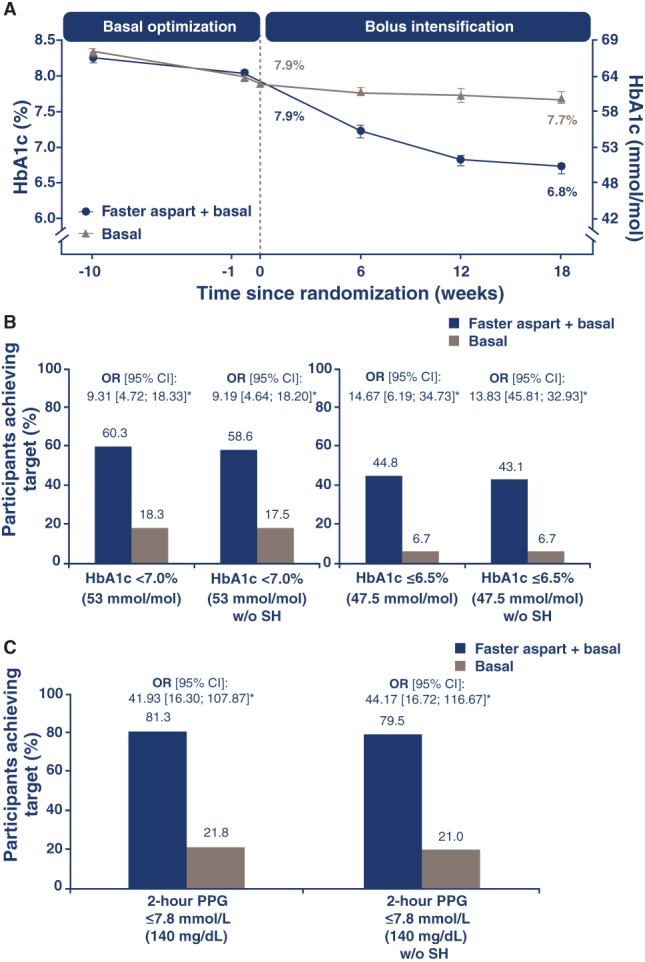
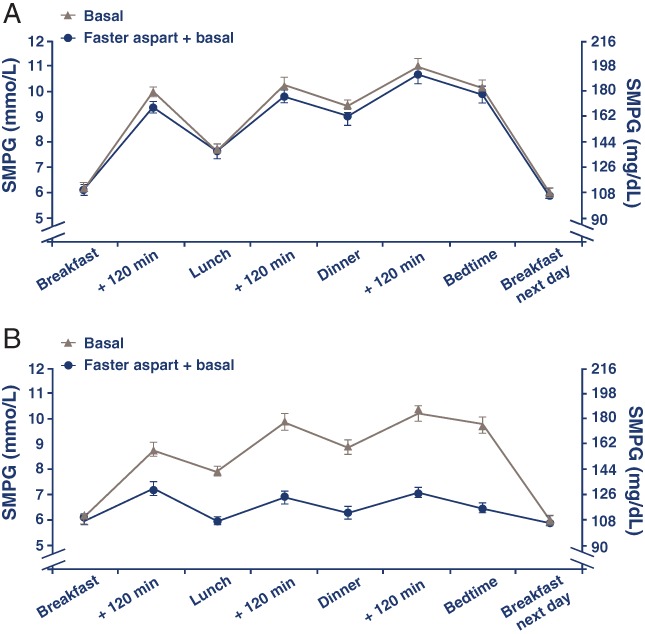
Materials and methods: In this open-label, randomized, 18-week trial (51 sites; 6 countries), adults (n = 236) with inadequately controlled type 2 diabetes (T2D; mean glycosylated haemoglobin [HbA1c] ± SD: 7.9% ± 0.7% [63.1 ± 7.5 mmol/mol]) receiving basal insulin and oral antidiabetic drugs underwent 8-week optimization of prior once-daily basal insulin followed by randomization 1:1 to either a BB regimen with faster aspart (n = 116) or continuation of once-daily basal insulin (n = 120), both with metformin. Primary endpoint was HbA1c change from baseline after 18 weeks of treatment. Secondary endpoints included: postprandial plasma glucose (PPG) change and overall PPG increment (all meals); weight; treatment-emergent adverse events; hypoglycaemic episodes.
Results: HbA1c decreased from 7.9% (63.2 mmol/mol) to 6.8% (50.7 mmol/mol; BB group) and from 7.9% (63.2 mmol/mol) to 7.7% (60.7 mmol/mol; basal-only group); estimated treatment difference [95% confidence interval] -0.94% [-1.17; -0.72]; -10.3 mmol/mol [-12.8; -7.8]; P < .0001. Reductions from baseline in overall mean 2-hour PPG and overall PPG increment for all meals (self-measured plasma glucose profiles) were statistically significant in favour of BB treatment ( P < .0001). Severe/blood glucose confirmed hypoglycaemia rate (12.8 vs 2.0 episodes per patient-years of exposure), total daily insulin (1.2 vs 0.6 U/kg) and weight gain (1.8 vs 0.2 kg) were greater with BB than with basal-only treatment.
Conclusions: In T2D, faster aspart in a BB regimen provided superior glycaemic control as compared with basal-only insulin, but with an increase in the frequency of hypoglycaemia and modest weight gain.
Trial registration: ClinicalTrials.gov NCT01850615.
Keywords: glycaemic control; hypoglycaemia; insulin therapy; phase 3 study; randomized trial; type 2 diabetes.
© 2017 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
H. W. R. reports receipt of grants and personal fees from AstraZeneca, Boehringer Ingelheim, Janssen, Lilly, Merck, Novo Nordisk, Sanofi and Regeneron. M. D. and S. T. are employees of Novo Nordisk. M. P. reports receipt of personal fees from Aventis, Lilly and Novo Nordisk. D. T. and M. V. V. have no conflicts of interest to disclose.
Figures
References
-
- Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient‐centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2015;38:140‐149. - PubMed
-
- American Diabetes Association . Standards of medical care in diabetes—2016: summary of revisions. Diabetes Care. 2016;39(suppl 1):S4‐S5. - PubMed
-
- International Diabetes Federation . Global Guideline for Type 2 Diabetes. Brussels, Belgium: International Diabetes Federation; 2012. http://www.idf.org/guideline‐type‐2‐diabetes. Accessed November 15, 2016.
-
- Raccah D, Bretzel RG, Owens D, Riddle M. When basal insulin therapy in type 2 diabetes mellitus is not enough what next? Diabetes Metab Res Rev. 2007;23:257‐264. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
