

Differentiation of Impaired From Preserved Hemodynamics in Patients With Fontan Circulation Using Real-time Phase-velocity Cardiovascular Magnetic Resonance
- PMID: 28346330
- PMCID: PMC5538303
- DOI: 10.1097/RTI.0000000000000261
Differentiation of Impaired From Preserved Hemodynamics in Patients With Fontan Circulation Using Real-time Phase-velocity Cardiovascular Magnetic Resonance
Abstract
Purpose: Progressive impairment of hemodynamics in patients with Fontan circulation is common, multifactorial, and associated with decreased quality of life and increased morbidity. We sought to assess hemodynamic differences between patients with preserved (preserved Fontans) and those with impaired circulation (impaired Fontans) after pulmonary vasodilation using oxygen and under forced breathing conditions.
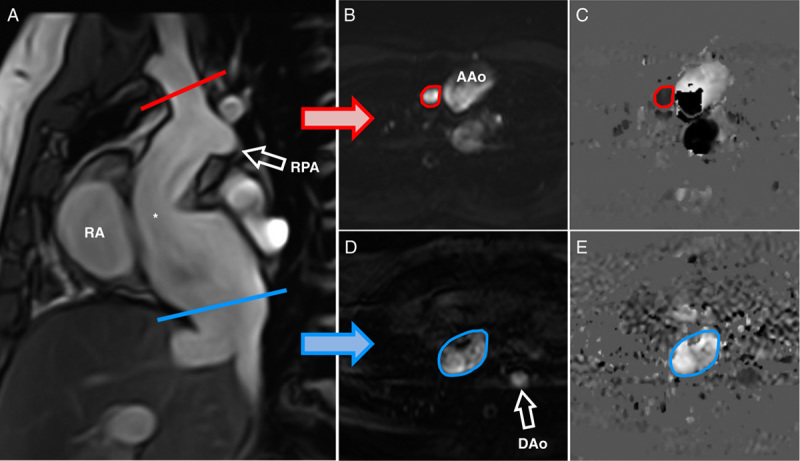
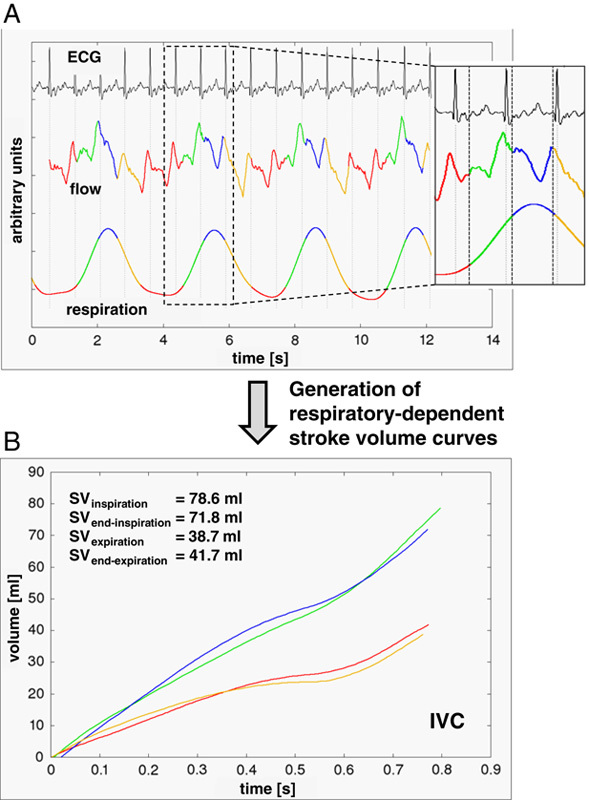
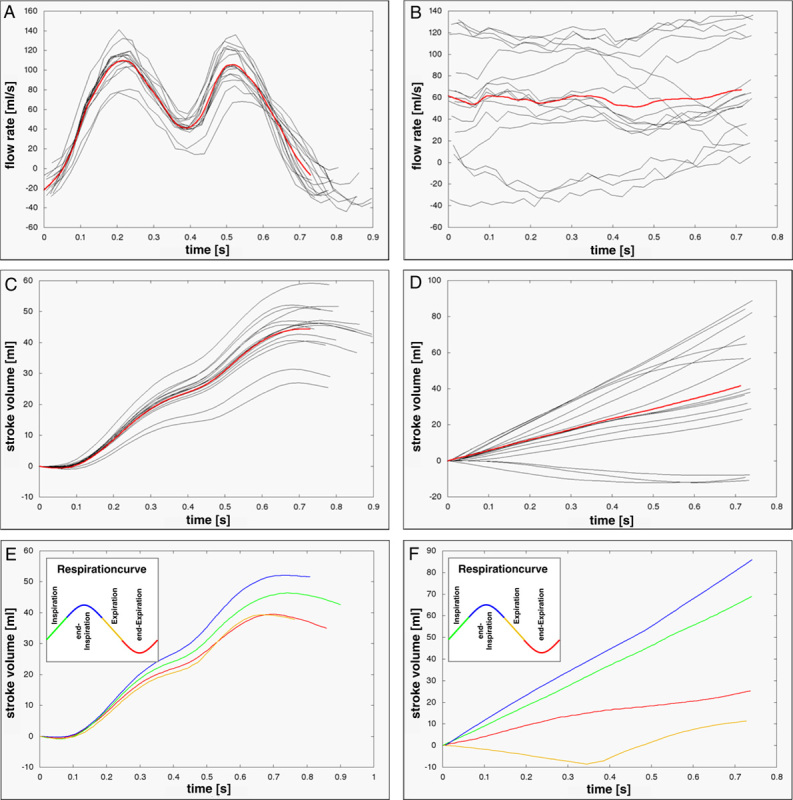
Materials and methods: Real-time phase-contrast cardiovascular magnetic resonance was performed using non-ECG triggered echo-planar imaging (temporal resolution=24 to 28 ms) in the ascending aorta (AAo) and superior vena cava (SVC)/inferior vena cava (IVC) on room air, after 100% oxygen inhalation (4 L/min; 10 min) and on forced breathing in 29 Fontan patients (17.2±7.3 y) and in 32 controls on room air (13.4±3.7 y). The simultaneously recorded patients' respiratory cycle was divided into 4 segments (expiration, end-expiration, inspiration, and end-inspiration) to generate respiratory-dependent stroke volumes (SVs). The imaging data were matched with physiological data and analyzed with home-made software.
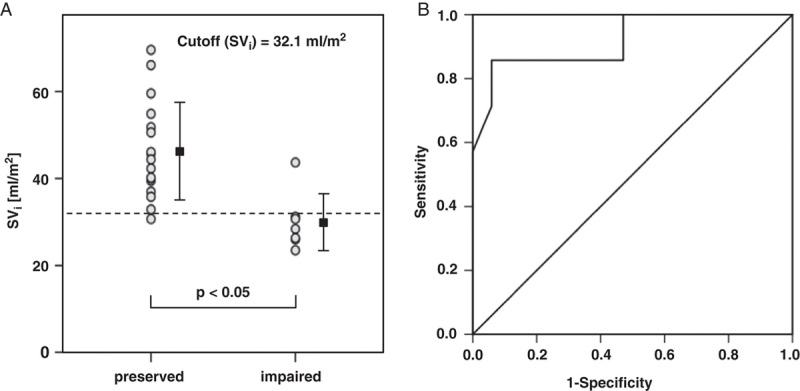
Results: The mean SVi (AAo) was 46.1±11.1 mL/m in preserved Fontans versus 30.4±6.2 mL/m in impaired Fontans (P=0.002) and 51.1±6.9 mL/m in controls (P=0.107). The cutoff value for differentiation of Fontan groups was SVi (AAo, end-expiratory) of 32.1 mL/m. After hyperoxygenation, the mean SVi (AAo) increased to 48.7±12.7 mL/m in preserved Fontans (P=0.045) but remained unchanged in impaired Fontans (31.1±5.8 mL/m, P=0.665). Simultaneously, heart rates decreased from 75.2±15.9 to 70.8±16.4 bpm (preserved; P=0.000) but remained unchanged in impaired circulation (baseline: 84.1±9.8 bpm, P=0.612). Compared with physiological respiration, forced breathing increased the maximum respiratory-related cardiac index difference (ΔCImax) in preserved Fontans (SVC: 2.5-fold, P=0.000; and IVC: 1.8-fold, P=0.000) and to a lower extent in impaired Fontans (both veins, 1.5-fold; P(SVC)=0.011, P(IVC)=0.013). There was no impact on mean blood flow.
Conclusions: Oxygen affected the pulmonary vascular system by vasodilation and increased SVi in preserved Fontans but had no effect on impaired Fontans. Forced breathing increased ΔCImax but did not change the mean blood flow by sole activation of the ventilatory pump. End-expiratory aortic SVi represents a valuable measure for classifying the severity of Fontan hemodynamics impairment.
Conflict of interest statement
Supported in part by the Fördergemeinschaft Deutsche Kinderherzzentren e.V.; Project identification No:W-BDO-019/2013. The authors declare no conflict of interest.
Figures
Similar articles
-
Impact of respiration on stroke volumes in paediatric controls and in patients after Fontan procedure assessed by MR real-time phase-velocity mapping.Eur Heart J Cardiovasc Imaging. 2015 Feb;16(2):198-209. doi: 10.1093/ehjci/jeu179. Epub 2014 Sep 21. Eur Heart J Cardiovasc Imaging. 2015. PMID: 25246504
-
Effect of Inhaled Nitric Oxide on Blood Flow Dynamics in Patients After the Fontan Procedure Using Cardiovascular Magnetic Resonance Flow Measurements.Pediatr Cardiol. 2016 Mar;37(3):504-11. doi: 10.1007/s00246-015-1307-1. Epub 2015 Nov 7. Pediatr Cardiol. 2016. PMID: 26547436
-
Caval flow reflects Fontan hemodynamics: quantification by magnetic resonance imaging.Clin Res Cardiol. 2012 Feb;101(2):133-8. doi: 10.1007/s00392-011-0374-4. Epub 2011 Nov 18. Clin Res Cardiol. 2012. PMID: 22094486
-
Respiratory Effects on Fontan Circulation During Rest and Exercise Using Real-Time Cardiac Magnetic Resonance Imaging.Ann Thorac Surg. 2016 May;101(5):1818-25. doi: 10.1016/j.athoracsur.2015.11.011. Epub 2016 Feb 10. Ann Thorac Surg. 2016. PMID: 26872728 Free PMC article.
-
Disintegration of the 'waterfall phenomenon' in the inferior vena cava due to right heart failure.Respirology. 1996 Mar;1(1):5-9. doi: 10.1111/j.1440-1843.1996.tb00005.x. Respirology. 1996. PMID: 9432406 Review.
Cited by
-
Impairments in Pulmonary Function in Fontan Patients: Their Causes and Consequences.Front Pediatr. 2022 Apr 15;10:825841. doi: 10.3389/fped.2022.825841. eCollection 2022. Front Pediatr. 2022. PMID: 35498782 Free PMC article. Review.
-
The Influence of Respiration on Blood Flow in the Fontan Circulation: Insights for Imaging-Based Clinical Evaluation of the Total Cavopulmonary Connection.Front Cardiovasc Med. 2021 Aug 5;8:683849. doi: 10.3389/fcvm.2021.683849. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34422920 Free PMC article. Review.
-
Real-Time Magnetic Resonance Imaging.J Magn Reson Imaging. 2022 Jan;55(1):81-99. doi: 10.1002/jmri.27411. Epub 2020 Dec 9. J Magn Reson Imaging. 2022. PMID: 33295674 Free PMC article. Review.
-
Validation and quantification of left ventricular function during exercise and free breathing from real-time cardiac magnetic resonance images.Sci Rep. 2022 Apr 4;12(1):5611. doi: 10.1038/s41598-022-09366-8. Sci Rep. 2022. PMID: 35379859 Free PMC article.
-
Respiration Dependency of Caval Blood Flow in Patients with Fontan Circulation: Quantification Using 5D Flow MRI.Radiol Cardiothorac Imaging. 2019 Oct 31;1(4):e190005. doi: 10.1148/ryct.2019190005. eCollection 2019 Oct. Radiol Cardiothorac Imaging. 2019. PMID: 33778515 Free PMC article.
References
-
- Rowland TW. The circulatory response to exercise: role of the peripheral pump. Int J Sports Med. 2001;22:558–565. - PubMed
-
- Cordina RL, O’Meagher S, Karmali A, et al. Resistance training improves cardiac output, exercise capacity and tolerance to positive airway pressure in Fontan physiology. Int J Cardiol. 2013;168:780–788. - PubMed
-
- De Vadder K, Van De Bruaene A, Gewillig M, et al. Predicting outcome after Fontan palliation: a single-centre experience, using simple clinical variables. Acta Cardiol. 2014;69:7–14. - PubMed
-
- de Leval MR. The Fontan circulation: a challenge to William Harvey? Nat Clin Pract Cardiovasc Med. 2005;2:202–208. - PubMed
-
- Bak Z, Sjoberg F, Rousseau A, et al. Human cardiovascular dose-response to supplemental oxygen. Acta Physiol (Oxf). 2007;191:15–24. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
