

Bacterial and viral pathogen spectra of acute respiratory infections in under-5 children in hospital settings in Dhaka city
- PMID: 28346512
- PMCID: PMC5367831
- DOI: 10.1371/journal.pone.0174488
Bacterial and viral pathogen spectra of acute respiratory infections in under-5 children in hospital settings in Dhaka city
Abstract
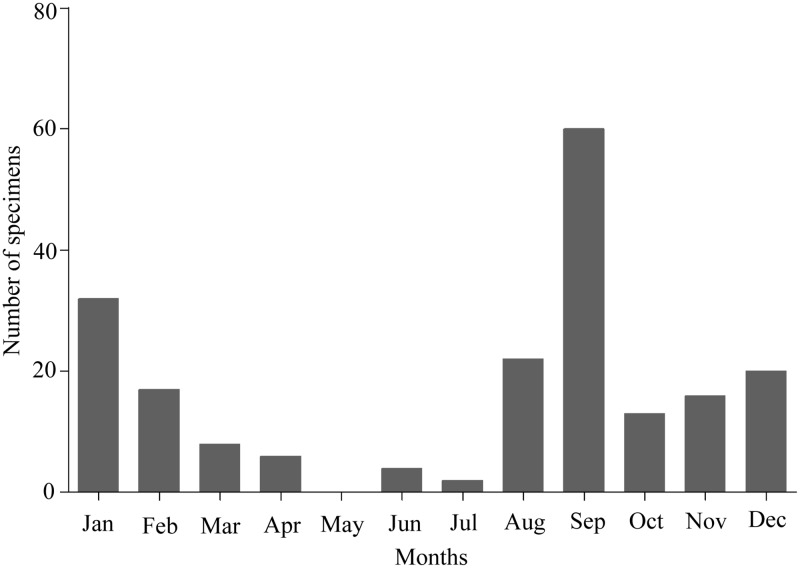
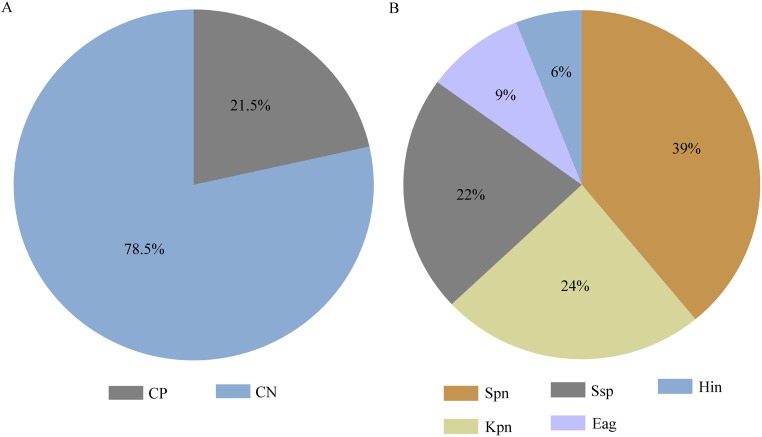
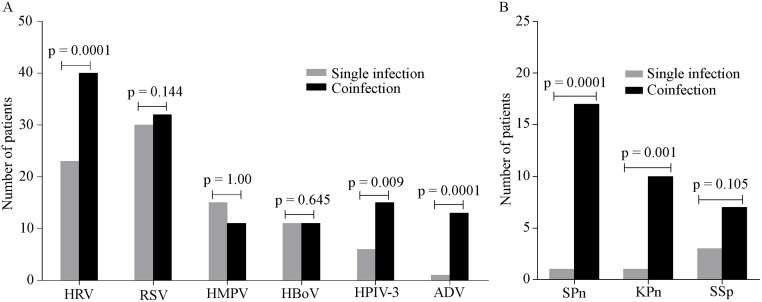
The study aimed to examine for the first time the spectra of viral and bacterial pathogens along with the antibiotic susceptibility of the isolated bacteria in under-5 children with acute respiratory infections (ARIs) in hospital settings of Dhaka, Bangladesh. Nasal swabs were collected from 200 under-five children hospitalized with clinical signs of ARIs. Nasal swabs from 30 asymptomatic children were also collected. Screening of viral pathogens targeted ten respiratory viruses using RT-qPCR. Bacterial pathogens were identified by bacteriological culture methods and antimicrobial susceptibility of the isolates was determined following CLSI guidelines. About 82.5% (n = 165) of specimens were positive for pathogens. Of 165 infected cases, 3% (n = 6) had only single bacterial pathogens, whereas 43.5% (n = 87) cases had only single viral pathogens. The remaining 36% (n = 72) cases had coinfections. In symptomatic cases, human rhinovirus was detected as the predominant virus (31.5%), followed by RSV (31%), HMPV (13%), HBoV (11%), HPIV-3 (10.5%), and adenovirus (7%). Streptococcus pneumoniae was the most frequently isolated bacterial pathogen (9%), whereas Klebsiella pneumaniae, Streptococcus spp., Enterobacter agglomerans, and Haemophilus influenzae were 5.5%, 5%, 2%, and 1.5%, respectively. Of 15 multidrug-resistant bacteria, a Klebsiella pneumoniae isolate and an Enterobacter agglomerans isolate exhibited resistance against more than 10 different antibiotics. Both ARI incidence and predominant pathogen detection rates were higher during post-monsoon and winter, peaking in September. Pathogen detection rates and coinfection incidence in less than 1-year group were significantly higher (P = 0.0034 and 0.049, respectively) than in 1-5 years age group. Pathogen detection rate (43%) in asymptomatic cases was significantly lower compared to symptomatic group (P<0.0001). Human rhinovirus, HPIV-3, adenovirus, Streptococcus pneumonia, and Klebsiella pneumaniae had significant involvement in coinfections with P values of 0.0001, 0.009 and 0.0001, 0.0001 and 0.001 respectively. Further investigations are required to better understand the clinical roles of the isolated pathogens and their seasonality.
Conflict of interest statement
Figures

References
-
- Organization WH. World health statistics 2010: WHO; 2010.
-
- Williams BG, Gouws E, Boschi-Pinto C, Bryce J, Dye C. Estimates of world-wide distribution of child deaths from acute respiratory infections. Lancet. Infect. Dis. 2002;2(1):25–32. - PubMed
-
- Sočan M, Marinič-Fišer N, Kraigher A, Kotnik A, Logar M. Microbial aetiology of community-acquired pneumonia in hospitalised patients. Eur. J. Clin. Microbiol. Infect. Dis. 1999;18(11):777–82. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
