

Patient-Reported Outcomes 1 Year After Immediate Breast Reconstruction: Results of the Mastectomy Reconstruction Outcomes Consortium Study
- PMID: 28346808
- PMCID: PMC5536162
- DOI: 10.1200/JCO.2016.69.9561
Patient-Reported Outcomes 1 Year After Immediate Breast Reconstruction: Results of the Mastectomy Reconstruction Outcomes Consortium Study
Abstract
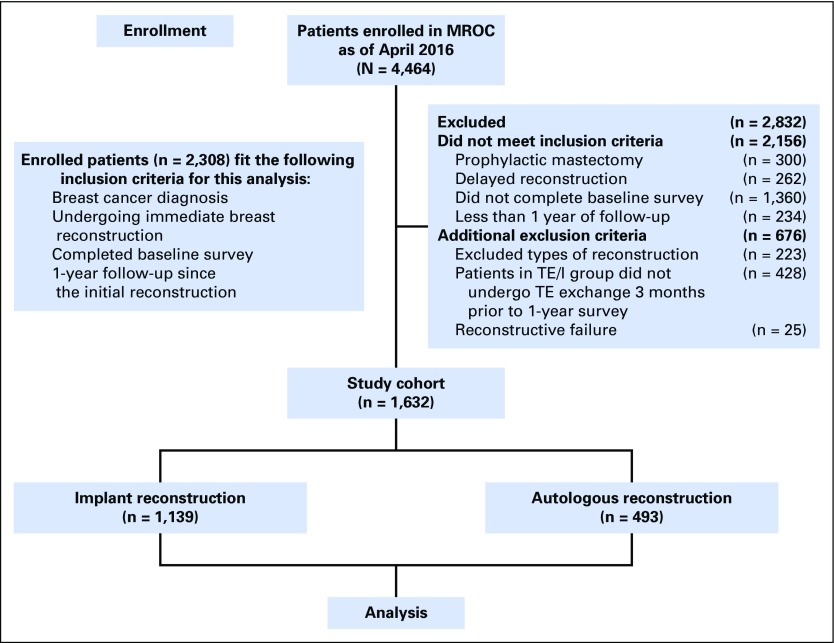
Purpose The goals of immediate postmastectomy breast reconstruction are to minimize deformity and optimize quality of life as perceived by patients. We prospectively evaluated patient-reported outcomes (PROs) in women undergoing immediate implant-based or autologous reconstruction. Methods Women undergoing immediate postmastectomy reconstruction for invasive cancer and/or carcinoma in situ were enrolled at 11 sites. Women underwent implant-based or autologous tissue reconstruction. Patients completed the BREAST-Q, a condition-specific PRO measure for breast surgery patients, and Patient-Reported Outcomes Measurement Information System-29, a generic PRO measure, before and 1 year after surgery. Mean changes in PRO scores were summarized. Mixed-effects regression models were used to compare PRO scores across procedure types. Results In total, 1,632 patients (n = 1,139 implant, n = 493 autologous) were included; 1,183 (72.5%) responded to 1-year questionnaires. After analysis was controlled for baseline values, patients who underwent autologous reconstruction had greater satisfaction with their breasts than those who underwent implant-based reconstruction (difference, 6.3; P < .001), greater sexual well-being (difference, 4.5; P = .003), and greater psychosocial well-being (difference, 3.7; P = .02) at 1 year. Patients in the autologous reconstruction group had improved satisfaction with breasts (difference, 8.0; P = .002) and psychosocial well-being (difference, 4.6; P = .047) compared with preoperative baseline. Physical well-being of the chest was not fully restored in either the implant group (difference, -3.8; P = .001) or autologous group (-2.2; P = .04), nor was physical well-being of the abdomen in patients who underwent autologous reconstruction (-13.4; P < .001). Anxiety and depression were mitigated at 1 year in both groups. Compared with their baseline reports, patients who underwent implant reconstruction had decreased fatigue (difference, -1.4; P = .035), whereas patients who underwent autologous reconstruction had increased pain interference (difference, 2.0; P = .006). Conclusion At 1 year after mastectomy, patients who underwent autologous reconstruction were more satisfied with their breasts and had greater psychosocial and sexual well-being than those who underwent implant reconstruction. Although satisfaction with breasts was equal to or greater than baseline levels, physical well-being was not fully restored. This information can help patients better understand expected outcomes and may guide innovations to improve outcomes.
Figures
References
-
- Surveillance, Epidemiology, and End Results (SEER): Cancer Statistics Review 1975–2009 (Vintage 2009 Populations). Bethesda, MD, National Cancer Institute, 2012.
-
- Kummerow KL, Du L, Penson DF, et al. Nationwide trends in mastectomy for early-stage breast cancer. JAMA Surg. 2015;150:9–16. - PubMed
-
- Portschy PR, Tuttle TM. Rise of mastectomy. J Surg Oncol. 2013;107:563–564. - PubMed
-
- Stucky CC, Gray RJ, Wasif N, et al. Increase in contralateral prophylactic mastectomy: Echoes of a bygone era? Surgical trends for unilateral breast cancer. Ann Surg Oncol. 2010;17:330–337. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
