

The association between sodium fluctuations and mortality in surgical patients requiring intensive care
- PMID: 28347943
- PMCID: PMC5679219
- DOI: 10.1016/j.jcrc.2017.02.012
The association between sodium fluctuations and mortality in surgical patients requiring intensive care
Abstract
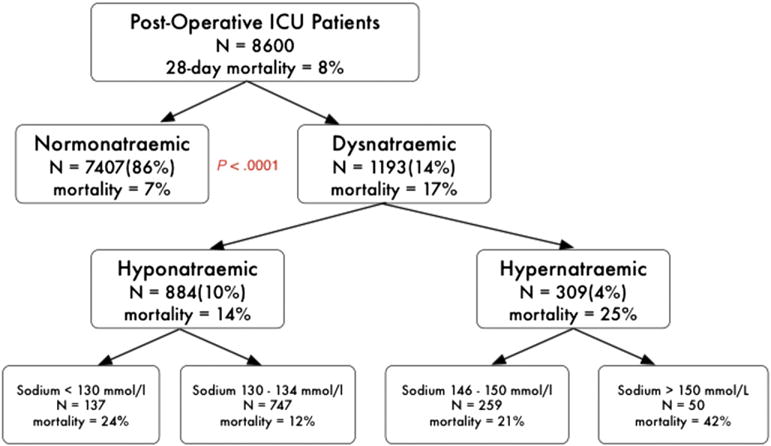
Purpose: Serum sodium derangement is the most common electrolyte disturbance among patients admitted to intensive care. This study aims to validate the association between dysnatremia and serum sodium fluctuation with mortality in surgical intensive care patients.
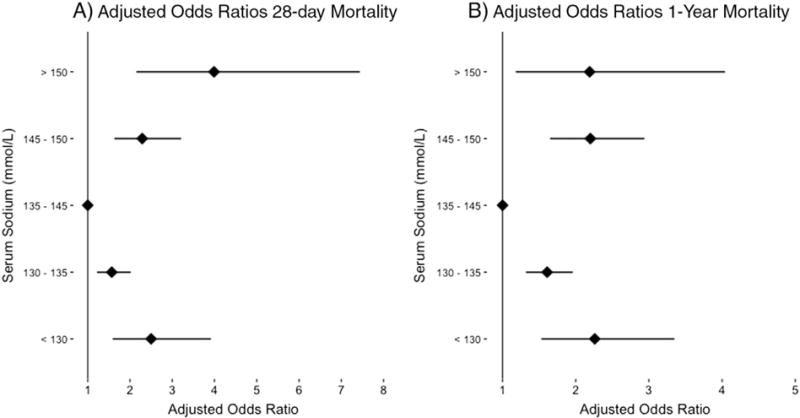
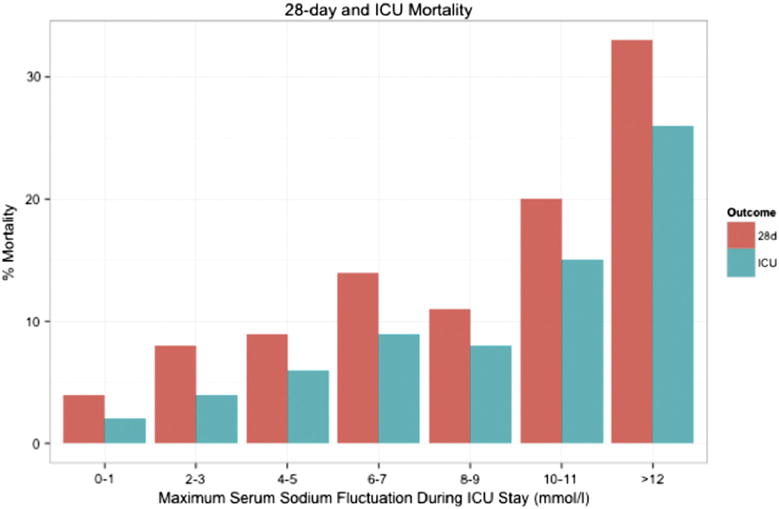
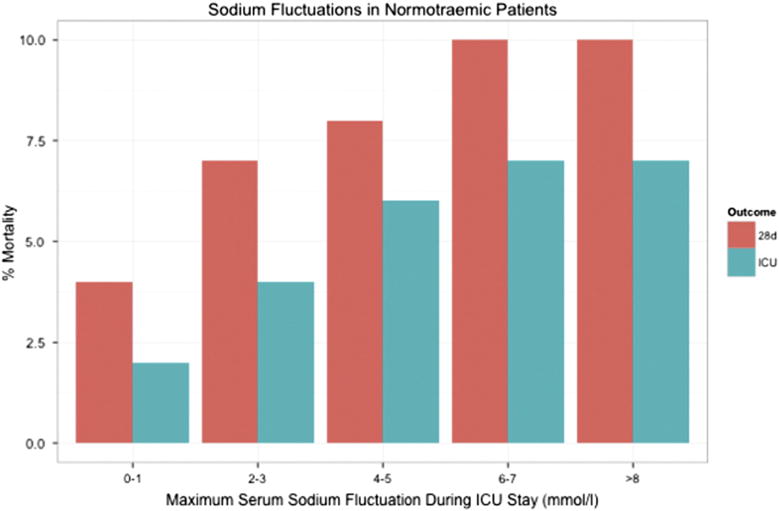
Method: We performed a retrospective analysis of the Medical Information Mart for Intensive Care II database. Dysnatremia was defined as a sodium concentration outside physiologic range (135-145mmol/L) and subjects were categorized by severity of dysnatremia and sodium fluctuation. Univariate and multivariable logistic regressions were used to test for associations between sodium fluctuations and mortality.
Results: We identified 8600 subjects, 39% of whom were female, with a median age of 66years for analysis. Subjects with dysnatremia were more likely to be dead at 28 days (17% vs 7%; P<.001). There was a significant association between sodium fluctuation and mortality at 28 days (adjusted odds ratio per 1mmol/L change, 1.10 [95% confidence interval, 1.08-1.12; P<.001]), even in patients who remained normotremic during their intensive care unit stay (1.12 [95% confidence interval, 1.09-1.16; P<.001]) CONCLUSIONS: This observational study validates previous findings of an association between serum sodium fluctuations and mortality in surgical intensive care patients. This association was also present in subjects who remained normonatremic throughout their intensive care unit admission.
Keywords: Dysnatremia; Electrolyte disturbances; Mortality; Sodium; Surgery.
Copyright © 2017. Published by Elsevier Inc.
Conflict of interest statement
Conflict of interest: The authors report no conflict of interest.
Figures
References
-
- Gennari FJ. Serum osmolality. N Engl J Med. 1984;310(2):102–5. - PubMed
-
- Funk G-C, Lindner G, Druml W, Metnitz B, Schwarz C, Bauer P, et al. Incidence and prognosis of dysnatremias present on ICU admission. Intensive Care Med. 2009;36(2):304–11. - PubMed
-
- Lindner G, Funk G-C, Schwarz C, Kneidinger N, Kaider A, Schneeweiss B, et al. Hypernatremia in the critically ill is an independent risk factor for mortality. Am J Kidney Dis. 2007;50(6):952–7. - PubMed
-
- Bennani S-L, Abouqal R, Zeggwagh A-A, Madani N, Abidi K, Zekraoui A, et al. Incidence, causes and prognostic factors of hyponatremia in intensive care. Rev Méd Interne. 2003;24(4):224–9. - PubMed
-
- Lenz K, Gössinger H, Laggner A, Druml W, Grimm G, Schneeweiss B. Influence of hypernatremic-hyperosmolar state on hemodynamics of patients with normal and depressed myocardial function. Crit Care Med. 1986;14(10):913–4. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
