

Association between Monocyte Count and Risk of Incident CKD and Progression to ESRD
- PMID: 28348030
- PMCID: PMC5383390
- DOI: 10.2215/CJN.09710916
Association between Monocyte Count and Risk of Incident CKD and Progression to ESRD
Abstract
Background and objectives: Experimental evidence suggests a role for monocytes in the biology of kidney disease progression; however, whether monocyte count is associated with risk of incident CKD, CKD progression, and ESRD has not been examined in large epidemiologic studies.
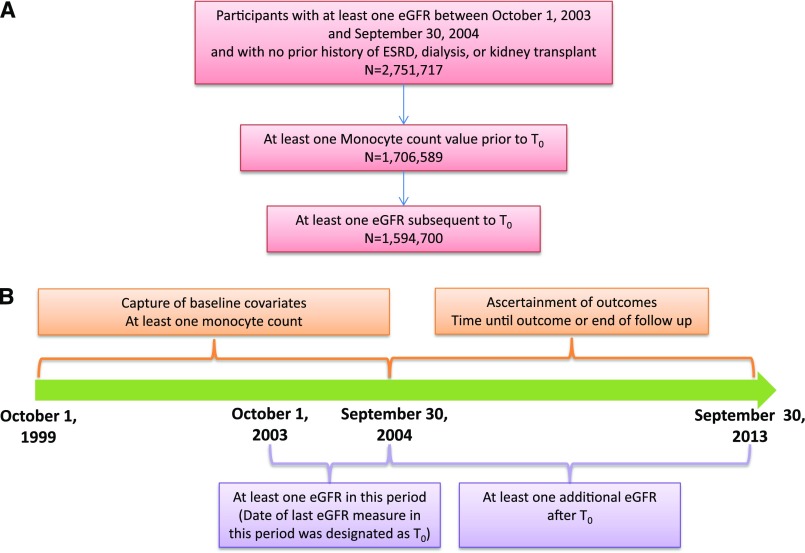
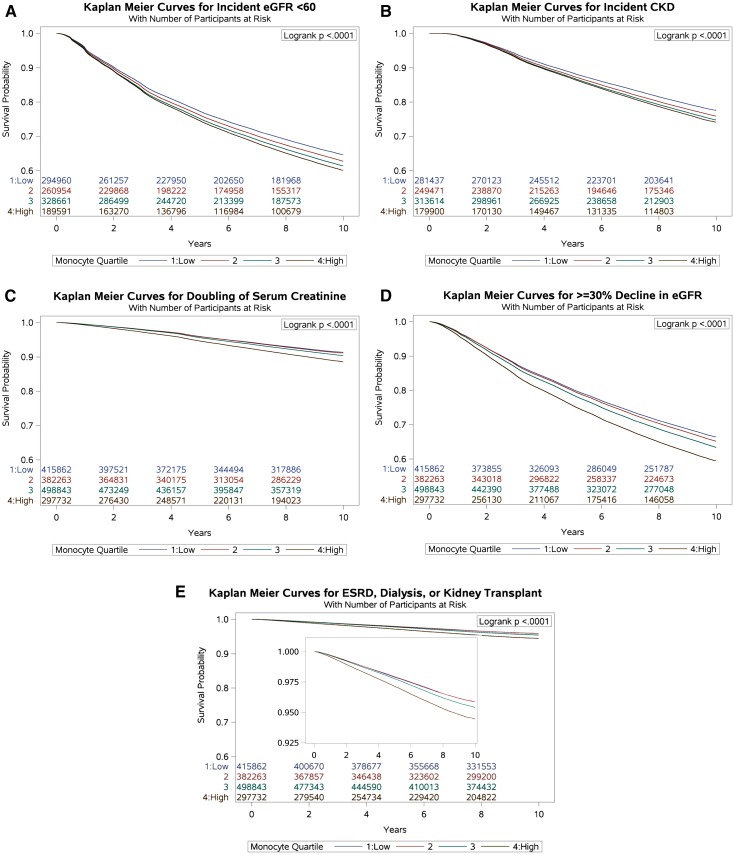
Design, settings, participants, & measurements: We built a longitudinal observational cohort of 1,594,700 United States veterans with at least one eGFR during fiscal year 2004 (date of last eGFR during this period designated time zero) and no prior history of ESRD, dialysis, or kidney transplant. Cohort participants were followed until September 30, 2013 or death. Monocyte count closest to and before time zero was categorized in quartiles: quartile 1, >0.00 to ≤0.40 thousand cells per cubic millimeter (k/cmm); quartile 2, >0.40 to ≤0.55 k/cmm; quartile 3, >0.55 to ≤0.70 k/cmm; and quartile 4, >0.70 k/cmm. Survival models were built to examine the association between monocyte count and risk of incident eGFR<60 ml/min per 1.73 m2, risk of incident CKD, and risk of CKD progression defined as doubling of serum creatinine, eGFR decline ≥30%, or the composite outcome of ESRD, dialysis, or renal transplantation.
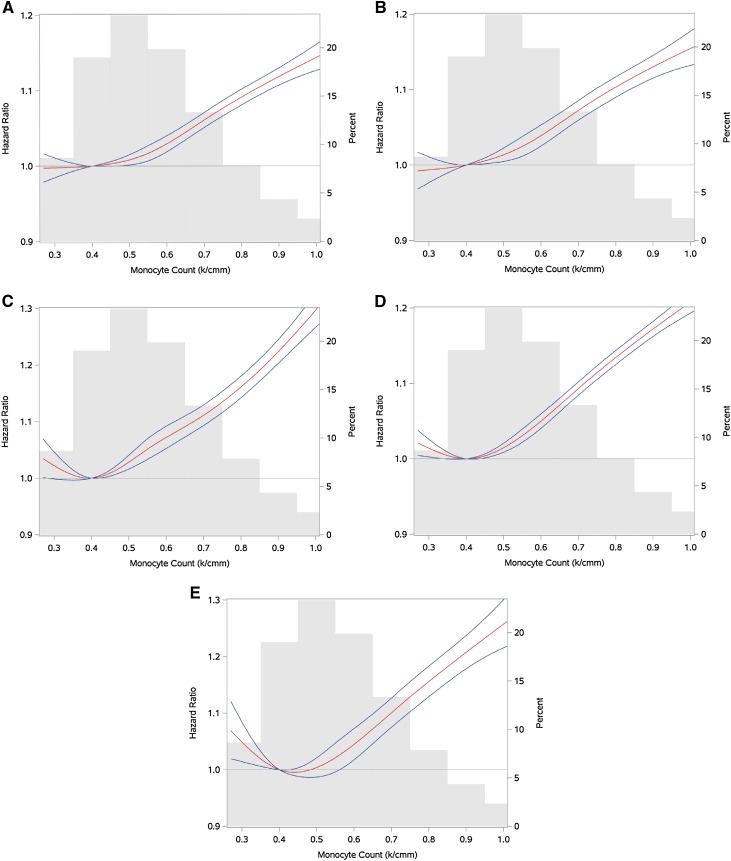
Results: Over a median follow-up of 9.2 years (interquartile range, 8.3-9.4); in adjusted survival models, there was a graded association between monocyte counts and risk of renal outcomes. Compared with quartile 1, quartile 4 was associated with higher risk of incident eGFR<60 ml/min per 1.73 m2 (hazard ratio, 1.13; 95% confidence interval, 1.12 to 1.14) and risk of incident CKD (hazard ratio, 1.15; 95% confidence interval, 1.13 to 1.16). Quartile 4 was associated with higher risk of doubling of serum creatinine (hazard ratio, 1.22; 95% confidence interval, 1.20 to 1.24), ≥30% eGFR decline (hazard ratio, 1.18; 95% confidence interval, 1.17 to 1.19), and the composite renal end point (hazard ratio, 1.19; 95% confidence interval, 1.16 to 1.22). Cubic spline analyses of the relationship between monocyte count levels and renal outcomes showed a linear relationship, in which risk was higher with higher monocyte count. Results were robust to changes in sensitivity analyses.
Conclusions: Our results show a significant association between higher monocyte count and risks of incident CKD and CKD progression to ESRD.
Keywords: Disease Progression; ESRD; Epidemiologic Studies; Epidemiology and outcomes; Follow-Up Studies; Kidney Failure, Chronic; Monocytes; Renal Insufficiency, Chronic; United States; Veterans; chemokine; chemokine receptor; chronic kidney disease; clinical epidemiology; creatinine; eGFR decline; eGFR slope; end stage kidney disease; kidney; kidney transplantation; renal dialysis; renal function decline; renal progression; white blood cell.
Copyright © 2017 by the American Society of Nephrology.
Figures
Similar articles
-
Low levels of high-density lipoprotein cholesterol increase the risk of incident kidney disease and its progression.Kidney Int. 2016 Apr;89(4):886-96. doi: 10.1016/j.kint.2015.12.034. Epub 2016 Jan 29. Kidney Int. 2016. PMID: 26924057
-
Monocyte count modifies the association between chronic kidney disease and risk of death .Clin Nephrol. 2018 Sep;90(3):194-208. doi: 10.5414/CN109434. Clin Nephrol. 2018. PMID: 29974856
-
Plasma Soluble Urokinase Plasminogen Activator Receptor (suPAR) and CKD Progression in Children.Am J Kidney Dis. 2020 Aug;76(2):194-202. doi: 10.1053/j.ajkd.2019.11.004. Epub 2020 Jan 24. Am J Kidney Dis. 2020. PMID: 31987488 Free PMC article.
-
Kidney Disease in Diabetes.In: Cowie CC, Casagrande SS, Menke A, Cissell MA, Eberhardt MS, Meigs JB, Gregg EW, Knowler WC, Barrett-Connor E, Becker DJ, Brancati FL, Boyko EJ, Herman WH, Howard BV, Narayan KMV, Rewers M, Fradkin JE, editors. Diabetes in America. 3rd edition. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases (US); 2018 Aug. CHAPTER 22. In: Cowie CC, Casagrande SS, Menke A, Cissell MA, Eberhardt MS, Meigs JB, Gregg EW, Knowler WC, Barrett-Connor E, Becker DJ, Brancati FL, Boyko EJ, Herman WH, Howard BV, Narayan KMV, Rewers M, Fradkin JE, editors. Diabetes in America. 3rd edition. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases (US); 2018 Aug. CHAPTER 22. PMID: 33651560 Free Books & Documents. Review.
-
Impact of Ramadan fasting on kidney function and related outcomes in chronic kidney disease and kidney transplant recipients: a systematic review and meta-analysis.BMJ Open. 2024 Nov 20;14(11):e085329. doi: 10.1136/bmjopen-2024-085329. BMJ Open. 2024. PMID: 39572100 Free PMC article.
Cited by
-
Myeloid cell-derived coagulation tissue factor is associated with renal tubular damage in mice fed an adenine diet.Sci Rep. 2021 Jun 9;11(1):12159. doi: 10.1038/s41598-021-91586-5. Sci Rep. 2021. PMID: 34108522 Free PMC article.
-
Is White Blood Cell Count Associated With Mortality in Peritoneal Dialysis Patients?: A Retrospective Single-Center Analysis.Cureus. 2021 Nov 18;13(11):e19728. doi: 10.7759/cureus.19728. eCollection 2021 Nov. Cureus. 2021. PMID: 34934591 Free PMC article.
-
Estimates of all cause mortality and cause specific mortality associated with proton pump inhibitors among US veterans: cohort study.BMJ. 2019 May 29;365:l1580. doi: 10.1136/bmj.l1580. BMJ. 2019. PMID: 31147311 Free PMC article.
-
Temporal trends of COVID-19 mortality and hospitalisation rates: an observational cohort study from the US Department of Veterans Affairs.BMJ Open. 2021 Aug 16;11(8):e047369. doi: 10.1136/bmjopen-2020-047369. BMJ Open. 2021. PMID: 34400452 Free PMC article.
-
Association of systemic inflammation response index with all-cause mortality as well as cardiovascular mortality in patients with chronic kidney disease.Front Cardiovasc Med. 2024 Feb 26;11:1363949. doi: 10.3389/fcvm.2024.1363949. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 38481957 Free PMC article.
References
-
- Ghattas A, Griffiths HR, Devitt A, Lip GY, Shantsila E: Monocytes in coronary artery disease and atherosclerosis: Where are we now? J Am Coll Cardiol 62: 1541–1551, 2013 - PubMed
-
- Swaminathan S, Shah SV: Novel inflammatory mechanisms of accelerated atherosclerosis in kidney disease. Kidney Int 80: 453–463, 2011 - PubMed
-
- Adamsson Eryd S, Smith JG, Melander O, Hedblad B, Engström G: Incidence of coronary events and case fatality rate in relation to blood lymphocyte and neutrophil counts. Arterioscler Thromb Vasc Biol 32: 533–539, 2012 - PubMed
-
- Johnsen SH, Fosse E, Joakimsen O, Mathiesen EB, Stensland-Bugge E, Njølstad I, Arnesen E: Monocyte count is a predictor of novel plaque formation: A 7-year follow-up study of 2610 persons without carotid plaque at baseline the Tromsø Study. Stroke 36: 715–719, 2005 - PubMed
-
- Nasir K, Guallar E, Navas-Acien A, Criqui MH, Lima JA: Relationship of monocyte count and peripheral arterial disease: Results from the National Health and Nutrition Examination Survey 1999-2002. Arterioscler Thromb Vasc Biol 25: 1966–1971, 2005 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
