

Portal hypertension: Imaging of portosystemic collateral pathways and associated image-guided therapy
- PMID: 28348478
- PMCID: PMC5352913
- DOI: 10.3748/wjg.v23.i10.1735
Portal hypertension: Imaging of portosystemic collateral pathways and associated image-guided therapy
Abstract
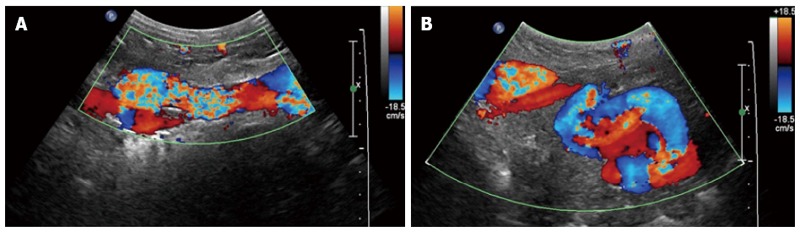
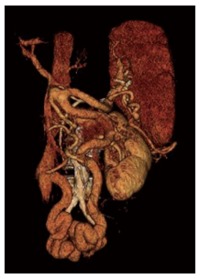
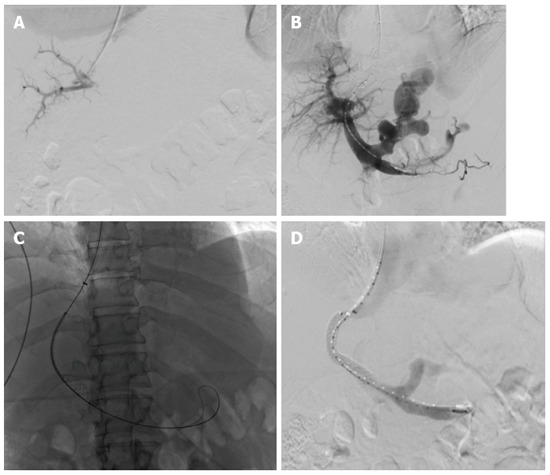
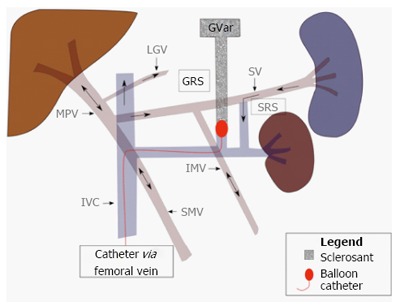
Portal hypertension is a common clinical syndrome, defined by a pathologic increase in the portal venous pressure. Increased resistance to portal blood flow, the primary factor in the pathophysiology of portal hypertension, is in part due to morphological changes occurring in chronic liver diseases. This results in rerouting of blood flow away from the liver through collateral pathways to low-pressure systemic veins. Through a variety of computed tomographic, sonographic, magnetic resonance imaging and angiographic examples, this article discusses the appearances and prevalence of both common and less common portosystemic collateral channels in the thorax and abdomen. A brief overview of established interventional radiologic techniques for treatment of portal hypertension will also be provided. Awareness of the various imaging manifestations of portal hypertension can be helpful for assessing overall prognosis and planning proper management.
Keywords: Diagnostic imaging; Image-guided therapy; Portal hypertension; Portosystemic collaterals.
Conflict of interest statement
Conflict-of-interest statement: Authors declare no potential conflicts of interests. No financial support.
Figures



References
-
- Bosch J, Abraldes JG, Fernández M, García-Pagán JC. Hepatic endothelial dysfunction and abnormal angiogenesis: new targets in the treatment of portal hypertension. J Hepatol. 2010;53:558–567. - PubMed
-
- Plessier A, Darwish-Murad S, Hernandez-Guerra M, Consigny Y, Fabris F, Trebicka J, Heller J, Morard I, Lasser L, Langlet P, et al. Acute portal vein thrombosis unrelated to cirrhosis: a prospective multicenter follow-up study. Hepatology. 2010;51:210–218. - PubMed
-
- Bosch J, Navasa M, Garcia-Pagán JC, DeLacy AM, Rodés J. Portal hypertension. Med Clin North Am. 1989;73:931–953. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
