

Tumoral Melanosis Associated with Pembrolizumab-Treated Metastatic Melanoma
- PMID: 28348944
- PMCID: PMC5348220
- DOI: 10.7759/cureus.1026
Tumoral Melanosis Associated with Pembrolizumab-Treated Metastatic Melanoma
Abstract
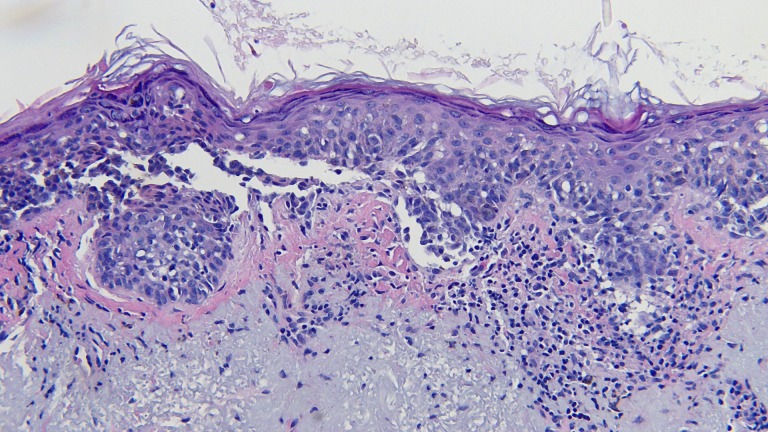
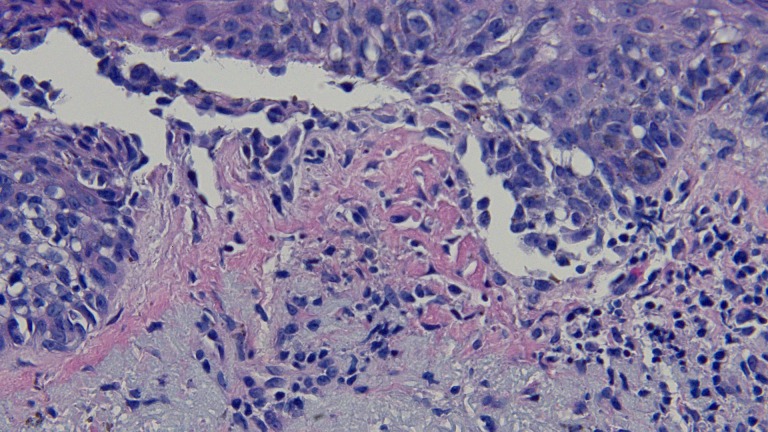
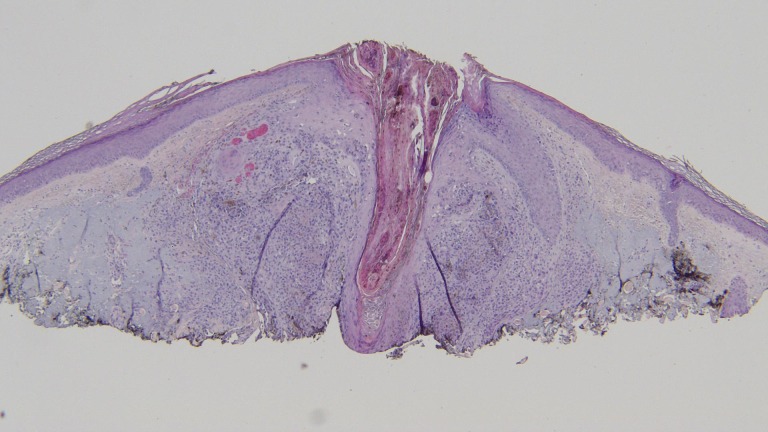
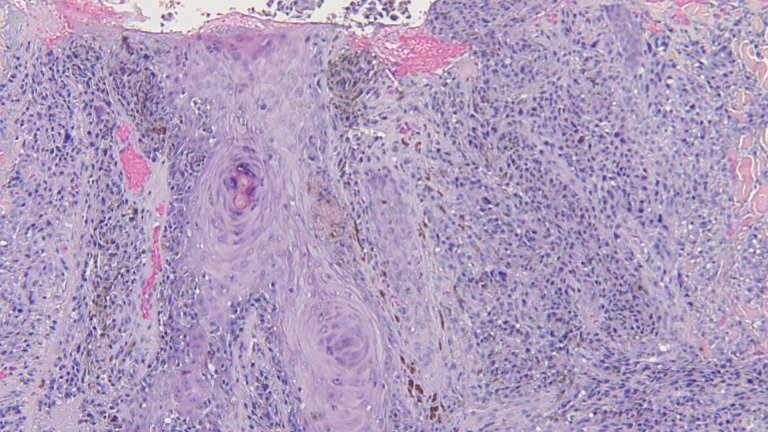
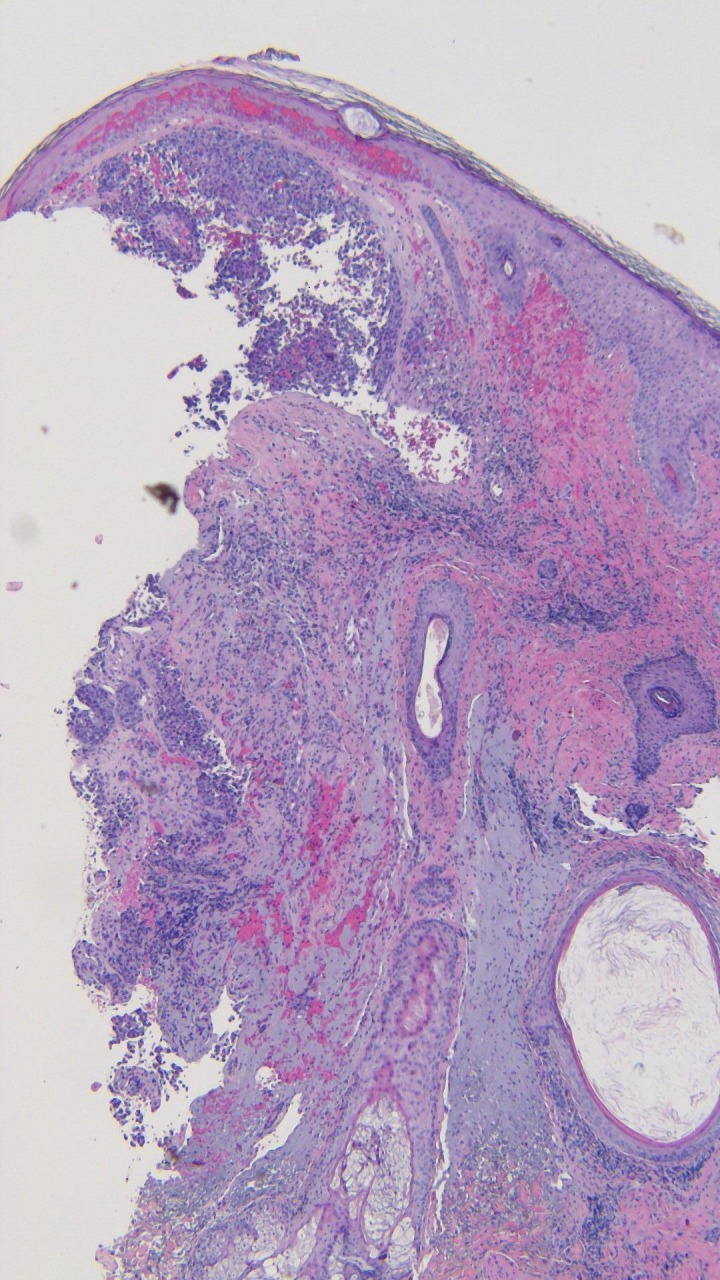
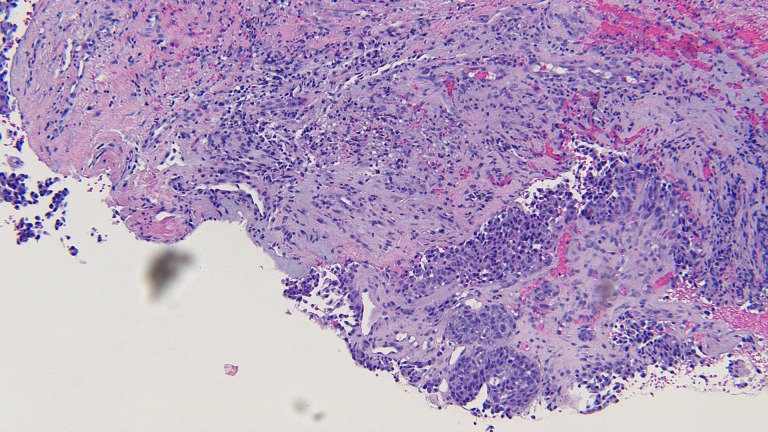
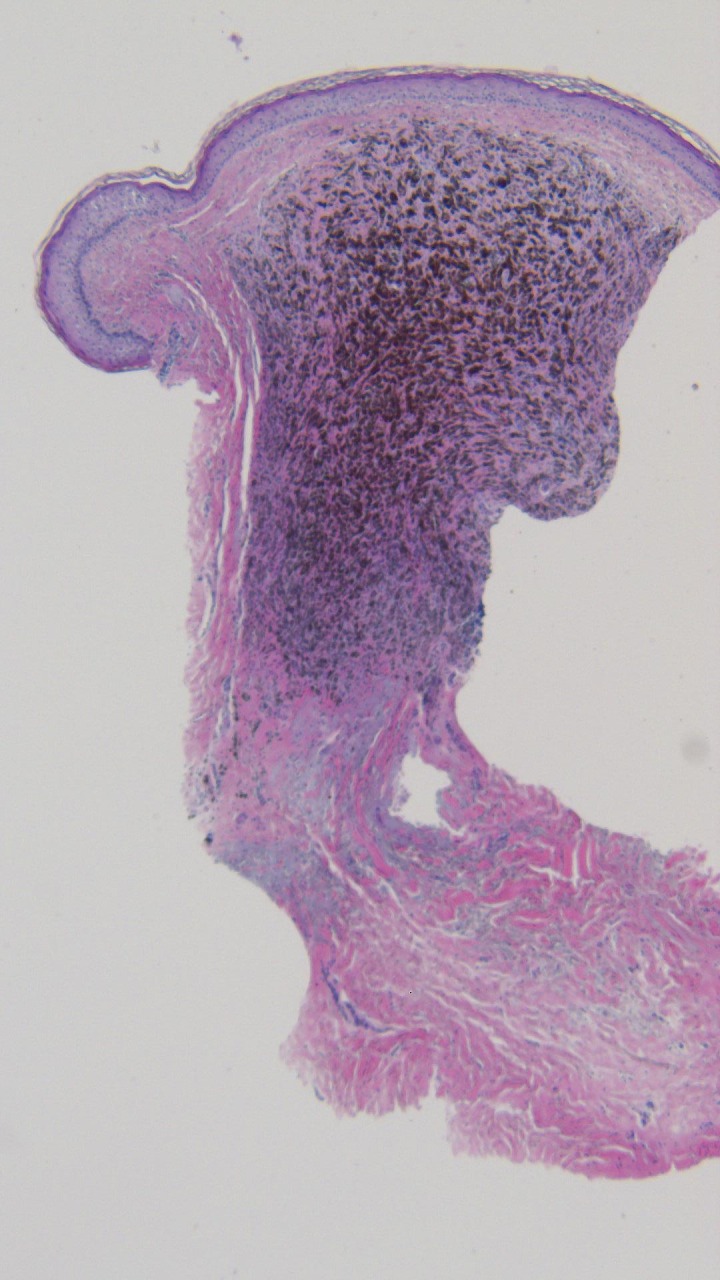
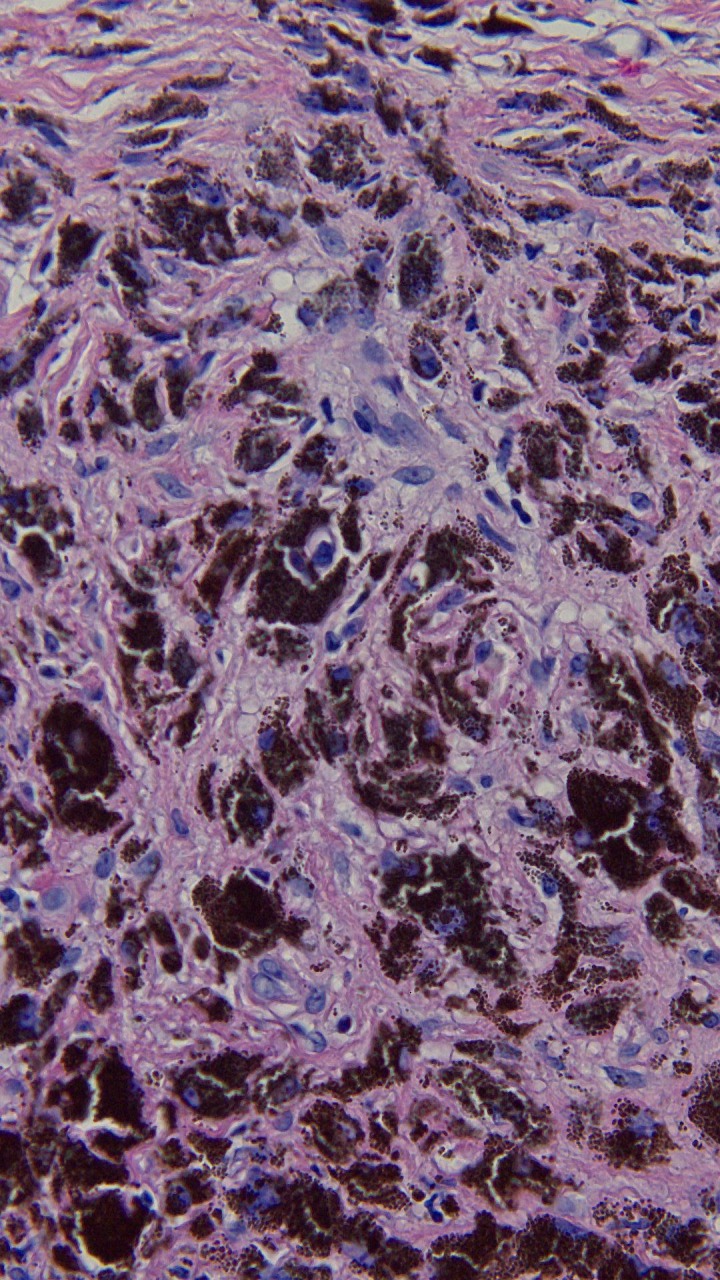
Tumoral melanosis is a form of completely regressed melanoma that usually presents as darkly pigmented lesions suspicious for malignant melanoma. Histology reveals dense dermal and subcutaneous infiltration of melanophages. Pembrolizumab is an antibody directed against programmed death receptor-1 (PD1) and is frontline treatment for advanced melanoma. An 81-year-old man with metastatic melanoma treated with pembrolizumab who developed tumoral melanosis at previous sites of metastases is described. The PubMed database was searched with the key words: antibody, immunotherapy, melanoma, melanosis, metastasis, pembrolizumab, and tumoral. The papers generated by the search and their references were reviewed. The patient was initially diagnosed with lentigo maligna melanoma on the left cheek three years earlier, and he was treated with wide local excision. The patient was subsequently diagnosed with epidermotropic metastatic malignant melanoma on the left parietal scalp 14 months later and was treated with wide local excision. Three months later, the patient was found to have metastatic melanoma in the same area of the scalp and was started on pembrolizumab immunotherapy. The patient was diagnosed with tumoral melanosis in the site of previous metastases nine months later. The patient remained free of disease 13 months after starting pembrolizumab. Tumoral melanosis may mimic malignant melanoma; hence a workup, including skin biopsy, should be undertaken. Extensive tumoral melanosis has been reported with ipilimumab, and we add a case following treatment with pembrolizumab. Additional cases of tumoral melanosis may present since immunotherapy has become frontline therapy for advanced melanoma.
Keywords: antibody; immunotherapy; melanoma; melanosis; metastasis; pembrolizumab; tumoral.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures






References
-
- Extensive tumoral melanosis associated with ipilimumab-treated melanoma. Staser K, Chen D, Solus J, et al. Br J Dermatol. 2016;175:391–393. - PubMed
-
- Melanophagic dermatitis and panniculitis. A condition revealing an occult metastatic malignant melanoma. Piérard GE. http://journals.lww.com/amjdermatopathology/Abstract/1988/04000/Melanoph.... Am J Dermatopathol. 1988;10:133–136. - PubMed
-
- Lymph node melanosis in a patient with metastatic melanoma of unknown primary. Malafronte P, Sorrells T. http://www.archivesofpathology.org/doi/full/10.1043/1543-2165-133.8.1332. Arch Pathol Lab Med. 2009;133:1332–1334. - PubMed
-
- Tumoral melanosis involving the sentinel lymph nodes: a case report. Satzger I, Völker B, Kapp A, Gutzmer R, et al. J Cutan Pathol. 2007;34:284–286. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources