

Amyloid-β accumulation in the CNS in human growth hormone recipients in the UK
- PMID: 28349199
- PMCID: PMC5508038
- DOI: 10.1007/s00401-017-1703-0
Amyloid-β accumulation in the CNS in human growth hormone recipients in the UK
Abstract
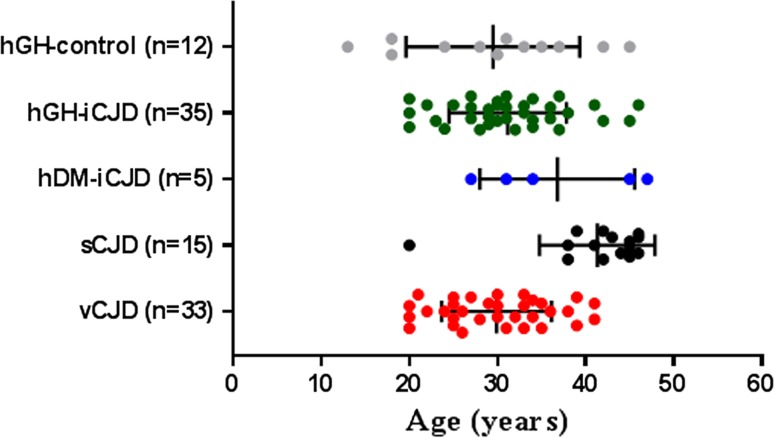
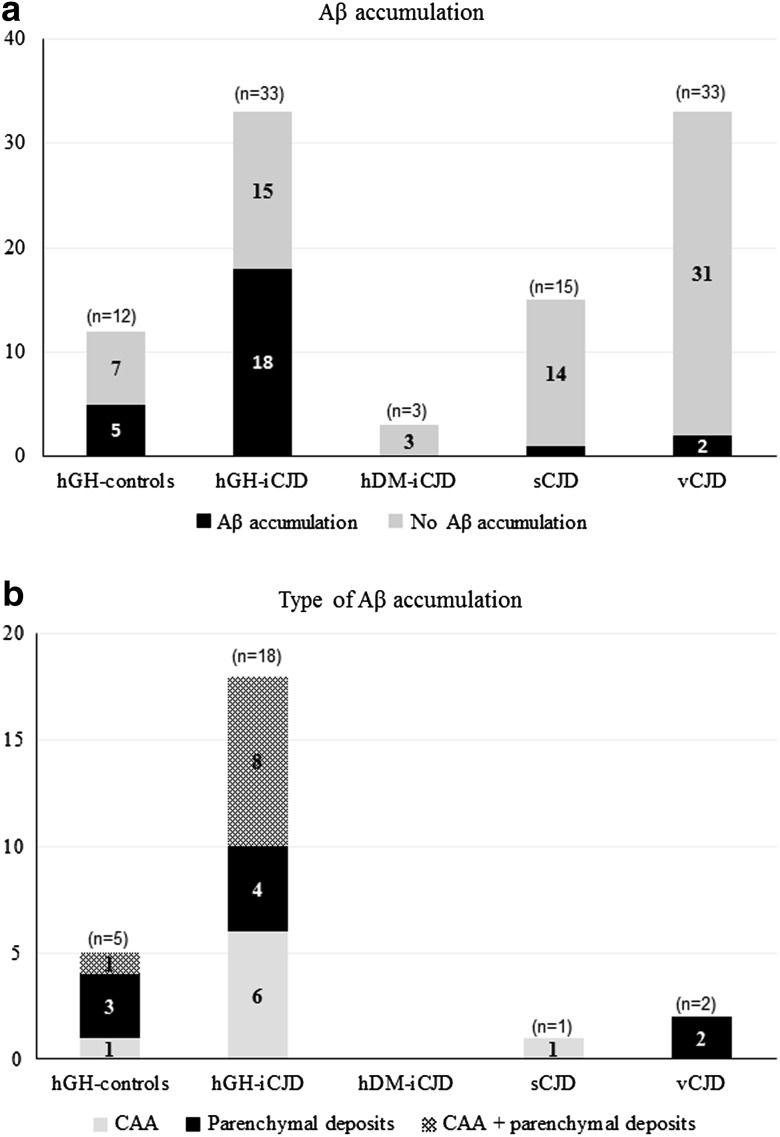
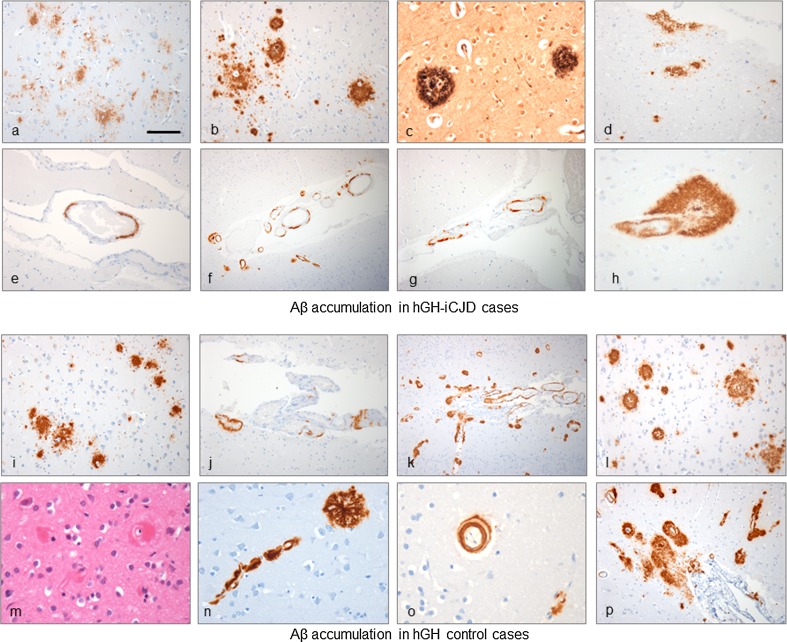
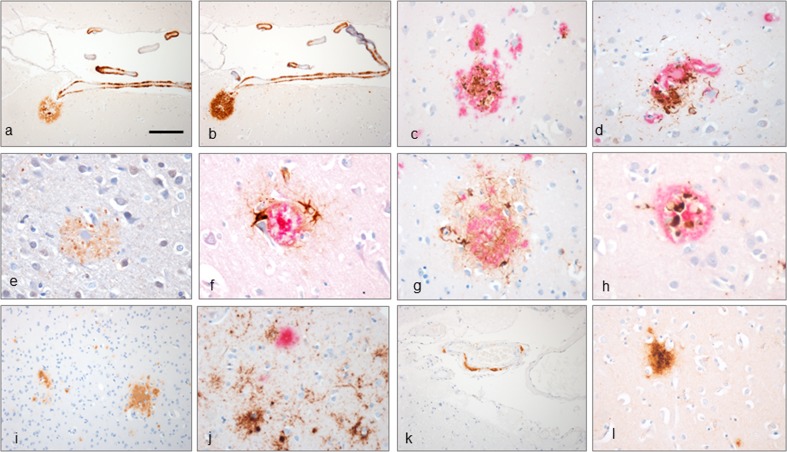
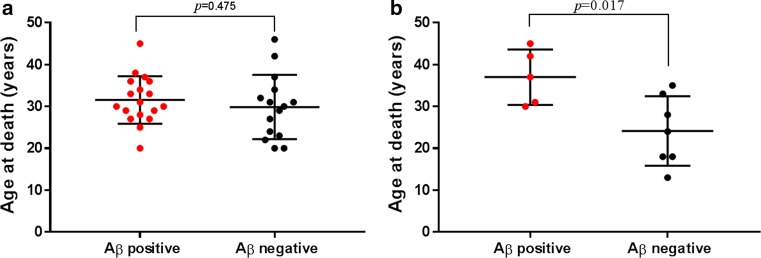
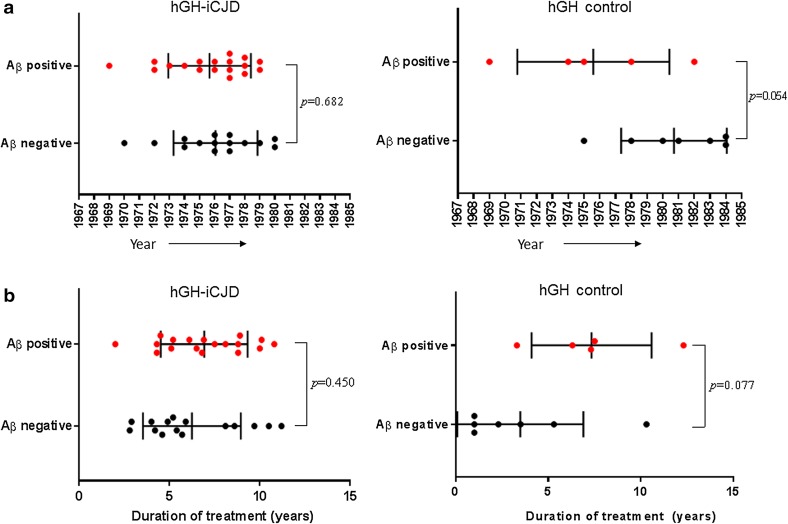
Human-to-human transmission of Creutzfeldt-Jakob disease (CJD) has occurred through medical procedures resulting in iatrogenic CJD (iCJD). One of the commonest causes of iCJD was the use of human pituitary-derived growth hormone (hGH) to treat primary or secondary growth hormone deficiency. As part of a comprehensive tissue-based analysis of the largest cohort yet collected (35 cases) of UK hGH-iCJD cases, we describe the clinicopathological phenotype of hGH-iCJD in the UK. In the 33/35 hGH-iCJD cases with sufficient paraffin-embedded tissue for full pathological examination, we report the accumulation of the amyloid beta (Aβ) protein associated with Alzheimer's disease (AD) in the brains and cerebral blood vessels in 18/33 hGH-iCJD patients and for the first time in 5/12 hGH recipients who died from causes other than CJD. Aβ accumulation was markedly less prevalent in age-matched patients who died from sporadic CJD and variant CJD. These results are consistent with the hypothesis that Aβ, which can accumulate in the pituitary gland, was present in the inoculated hGH preparations and had a seeding effect in the brains of around 50% of all hGH recipients, producing an AD-like neuropathology and cerebral amyloid angiopathy (CAA), regardless of whether CJD neuropathology had occurred. These findings indicate that Aβ seeding can occur independently and in the absence of the abnormal prion protein in the human brain. Our findings provide further evidence for the prion-like seeding properties of Aβ and give insights into the possibility of iatrogenic transmission of AD and CAA.
Keywords: Amyloid β; Cerebral amyloid angiopathy; Human growth hormone; Iatrogenic Creutzfeldt–Jakob disease; Neuropathology; Prion protein.
Conflict of interest statement
The authors declare that they have no conflicts of interest. The human tissue examined in this study was provided by the MRC Edinburgh Brain Bank and its use was covered by ethical approval from the East of Scotland Research Ethics Service REC 1 (reference number 16/ES/0084). Informed consent for the research use of autopsy tissue was obtained from the relatives of the deceased whenever necessary. This article does not contain any studies with animals performed by any of the authors.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
