

Intraoral Salivary Duct Cyst: Clinical and Histopathologic Features of 177 Cases
- PMID: 28349371
- PMCID: PMC5677068
- DOI: 10.1007/s12105-017-0810-5
Intraoral Salivary Duct Cyst: Clinical and Histopathologic Features of 177 Cases
Abstract
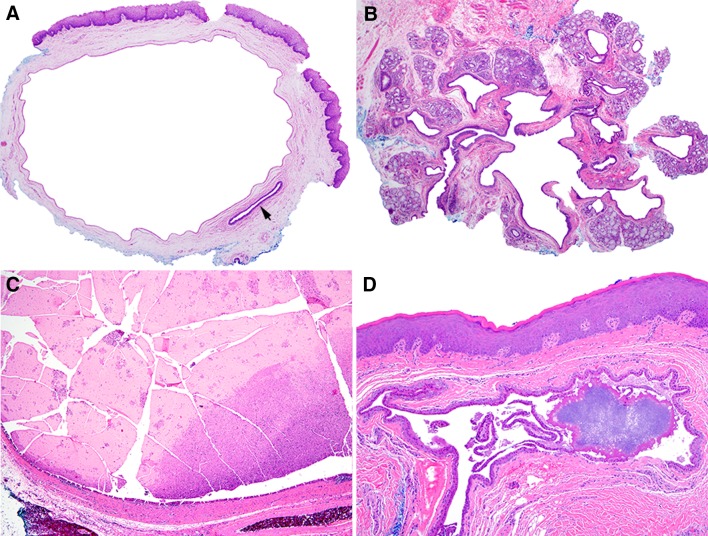
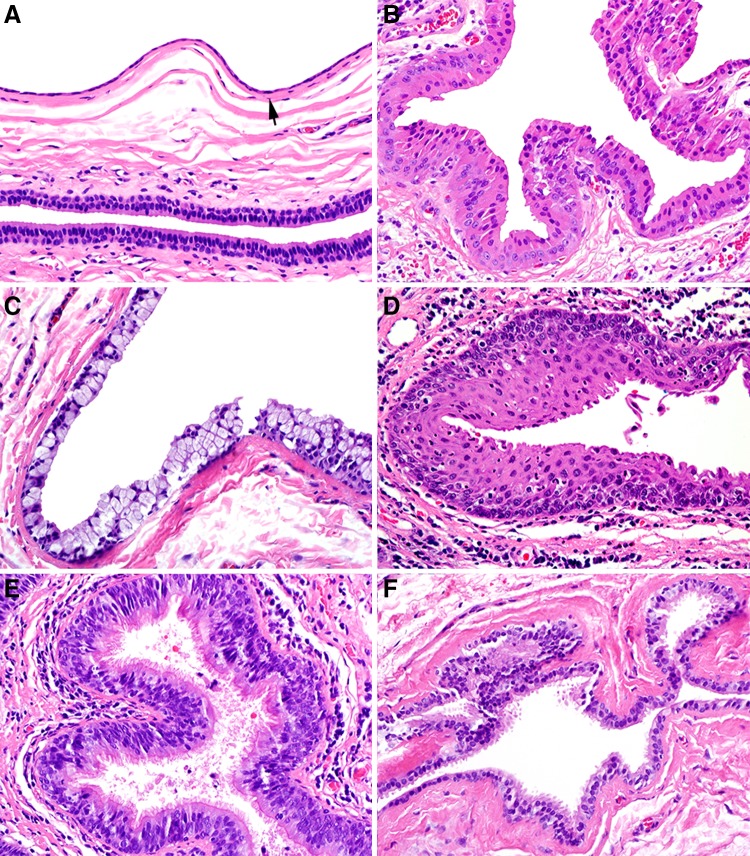
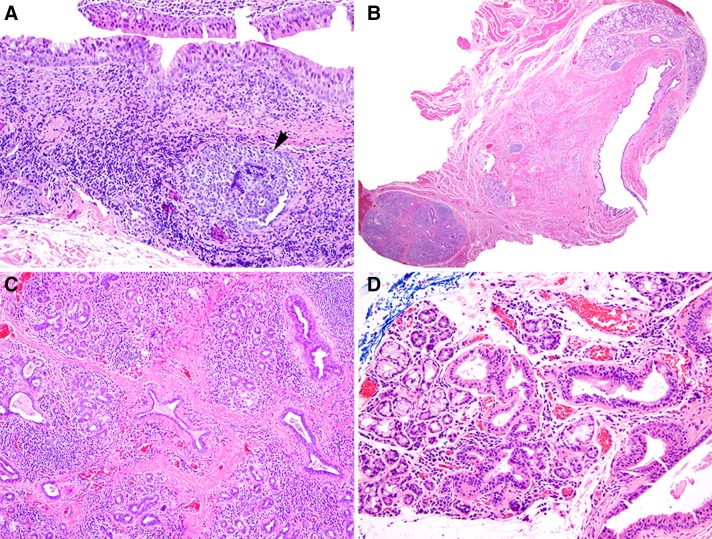
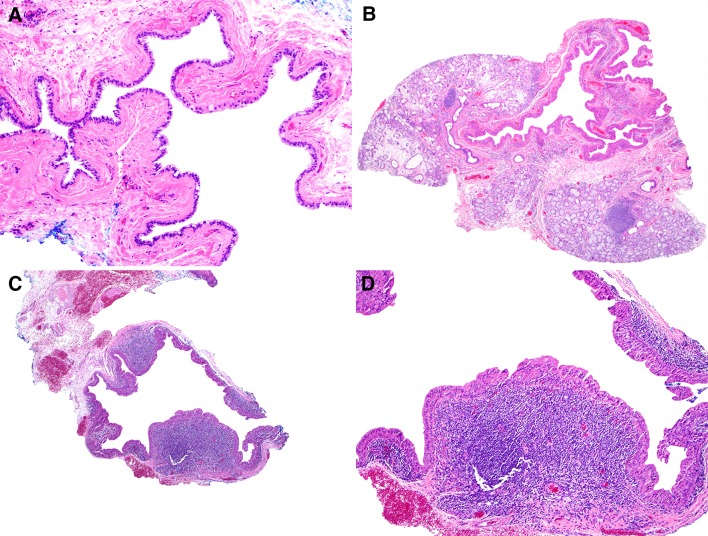
The salivary duct cyst (SDC) is a reactive ductal ectasia most frequently seen in major salivary glands, and likely caused by obstruction. The aim of this study is to define the clinical and histopathologic spectrum of intraoral SDCs. Cases were retrieved from the archives of Harvard School of Dental Medicine/StrataDx, Inc. from January 2012 to August 2014. There were 177 cases of which 103 (58.2%) occurred in females, with a median age of 56 (range 2-95). Approximately half of cases (45.8%) presented in the area of the buccal mucosa, lower lip mucosa, or mandibular vestibule, and 23.2% presented in the floor of mouth. SDCs were lined at least focally by 1-2 layers of cuboidal/columnar epithelium in 85.3% of cases and showed varying degrees of metaplasia (oncocytic, mucous cell, squamous, ciliated, apocrine-like) in 68.4% of cases. Intraluminal mucous stasis was present in 41.8% of SDCs, incipient calcification was present within 4.5% of SDCs, and chronic obstructive sialadenitis was seen in 90.2% of cases. No cysts showed adenomatous ductal proliferations or true papillary structures with fibrovascular cores, although 41.2% exhibited reactive undulation of cyst lining. Thirty-nine 'papillary oncocytic cystadenoma-like' SDCs (22.0%) demonstrated complete oncocytic metaplasia and marked undulation. An additional seven such cysts (4.0%) had a 'Warthin tumor-like' lymphoplasmacytic infiltrate. Intraoral SDCs occur most commonly in the sixth decade of life in locations distinct from extravasation mucoceles, likely secondary to intraluminal obstruction. SDCs show diverse histopathology and certain phenotypic variants may be mistaken for papillary oncocytic cystadenoma or Warthin tumor.
Keywords: Cystadenoma; Mucocele; Mucous retention cyst; Salivary duct cyst; Sialocyst; Warthin tumor.
Conflict of interest statement
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed Consent
Informed consent was not obtained as this study consists of secondary research performed on excess tissue of specimens used for diagnostic purposes. Research was conducted using deidentified samples and private patient information was not accessed at any point during the design of the study, data collection/interpretation, or manuscript preparation.
Figures

References
-
- Work WP Cysts and congenital lesions of the parotid gland. Otolaryngol Clin North Am. 1977;10(2):339–343. - PubMed
-
- Ellis GL, Auclair PL, American Registry of Pathology. Armed Forces Institute of Pathology(U.S.) Tumors of the salivary glands. AFIP atlas of tumor pathology Fourth series. Washington, DC: American Registry of Pathology in collaboration with the Armed Forces Institute of Pathology; 2008.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
