

NUT Midline Carcinoma of the Sublingual Gland: Clinical Presentation and Review
- PMID: 28349372
- PMCID: PMC5677058
- DOI: 10.1007/s12105-017-0809-y
NUT Midline Carcinoma of the Sublingual Gland: Clinical Presentation and Review
Abstract
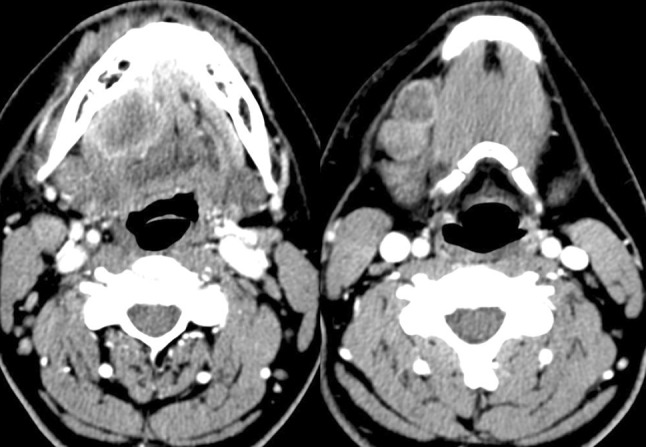
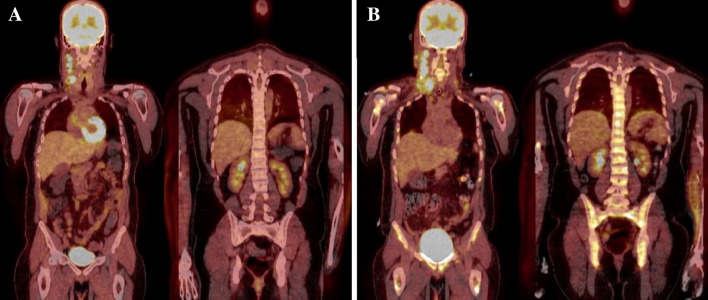
NUT midline carcinoma (NMC) is a rare and aggressive disease encountered in the midline of the head and neck or mediastinum. Due to its sparse incidence and subtle pathologic features, we aim to increase knowledge and awareness for this pathologic entity. We present an exemplary case of a young, healthy male presenting with oral cavity pain and cervical lymphadenopathy. This patient was initially diagnosed with an unspecified, highly aggressive sublingual gland malignancy and underwent locoregional resection with free flap reconstruction however suffered a rapid local recurrence and widely extensive metastasis within just 1 month. After rigorous analysis, final pathologic diagnosis revealed a poorly differentiated carcinoma with evidence of squamous differentiation that eventually, post-mortem tested positive for NMC. Only one prior case of sublingual gland NMC has been previously reported as we discuss the literature regarding all sublingual gland malignancies as well as the pathologic features and treatment options for NMC. We recommend consideration of testing for the NUT proto-oncogene at the time of biopsy in the clinical setting of a poorly differentiated midline carcinoma, especially with squamous differentiation, of the head or neck in order to identify patients for clinical trial enrollment and appropriately counsel on the poor clinical prognosis. Improving clinician awareness is critical to increase diagnostic accuracy and need to study prospective treatment outcomes as the first step toward improving management of this difficult disease.
Keywords: Floor of mouth; Head and neck cancer; Oral cancer; Sublingual salivary gland; Undifferentiated carcinoma.
Conflict of interest statement
Conflict of interest
Nolan Seim declares that he has no conflict of interest. Ramez Phillips declares he has no conflict of interest. Lynn Schoenfield declares that she has no conflict of interest. Theodoros Teknos declares that he has no conflict of interest. James Rocco declares that he has no conflict of interest. Amit Agrawal declares that he has no conflict of interest. Enver Ozer declares that he has no conflict of interest. Ricardo Carrau declares that he has no conflict of interest. Stephen Kang declares that he has no conflict of interest. Matthew Old declares that he has no conflict of interest.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed Consent
Not indicated for this study.
Figures

References
-
- Rutt AL, Hawkshaw MJ, Lurie D, Sataloff RT. Salivary gland cancer in patients younger than 30years. Ear Nose Throat J. 2011;90(4):174–184. - PubMed
-
- Andersen LJ, Therkildsen MH, Ockelmann HH, Bentzen JD, Schiødt T, Hansen HS. Malignant epithelial tumors in the minor salivary glands, the submandibular gland, and the sublingual gland. Prognostic factors and treatment results. Cancer. 1991;68(11):2431–2437. doi: 10.1002/1097-0142(19911201)68:11<2431::AID-CNCR2820681118>3.0.CO;2-N. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
