

Fresh versus frozen embryo transfers in assisted reproduction
- PMID: 28349510
- PMCID: PMC6464515
- DOI: 10.1002/14651858.CD011184.pub2
Fresh versus frozen embryo transfers in assisted reproduction
Update in
-
Fresh versus frozen embryo transfers in assisted reproduction.Cochrane Database Syst Rev. 2021 Feb 4;2(2):CD011184. doi: 10.1002/14651858.CD011184.pub3. Cochrane Database Syst Rev. 2021. PMID: 33539543 Free PMC article.
Abstract
Background: In general, in vitro fertilisation (IVF) or intracytoplasmic sperm injection (ICSI) implies a single fresh and one or more frozen-thawed embryo transfers. Alternatively, the 'freeze-all' strategy implies transfer of frozen-thawed embryos only, with no fresh embryo transfers. In practice, both strategies can vary technically including differences in freezing techniques and timing of transfer of cryopreservation, that is vitrification versus slow freezing, freezing of two pro-nucleate (2pn) versus cleavage-stage embryos versus blastocysts, and transfer of cleavage-stage embryos versus blastocysts.In the freeze-all strategy, embryo transfers are disengaged from ovarian stimulation in the initial treatment cycle. This could avoid a negative effect of ovarian hyperstimulation on the endometrium and thereby improve embryo implantation. It could also reduce the risk of ovarian hyperstimulation syndrome (OHSS) in the ovarian stimulation cycle by avoiding a pregnancy.We compared the benefits and risks of the two treatment strategies.
Objectives: To evaluate the effectiveness and safety of the freeze-all strategy compared to the conventional IVF/ICSI strategy in women undergoing assisted reproductive technology.
Search methods: We searched the Cochrane Gynaecology and Fertility Group Trials Register, the Cochrane Central Register of Studies (CRSO), MEDLINE, Embase, PsycINFO, CINAHL, and two registers of ongoing trials in November 2016 together with reference checking and contact with study authors and experts in the field to identify additional studies.
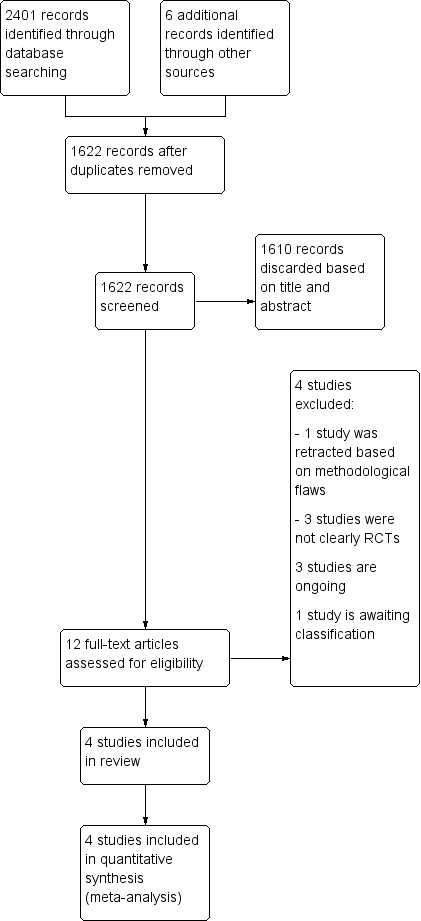
Selection criteria: We included randomised clinical trials comparing a freeze-all strategy with a conventional IVF/ICSI strategy which includes fresh transfer of embryos in women undergoing IVF or ICSI treatment.
Data collection and analysis: We used standard methodological procedures recommended by Cochrane. The primary review outcomes were cumulative live birth and OHSS. Secondary outcomes included other adverse effects (miscarriage rate).
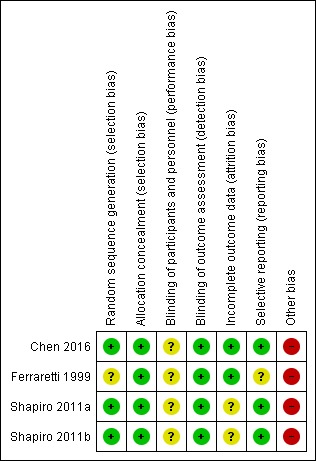
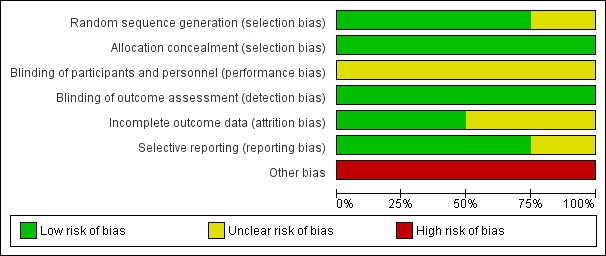
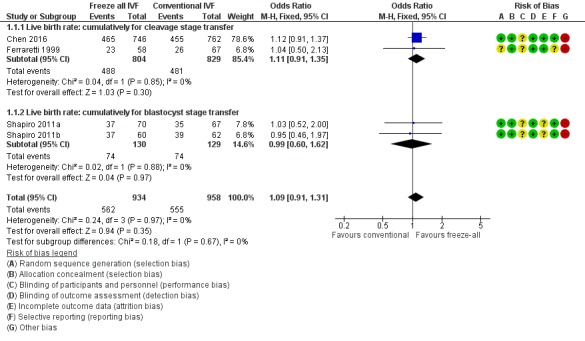
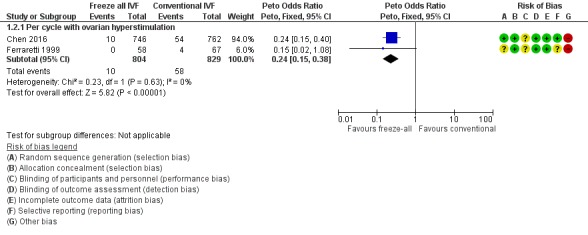
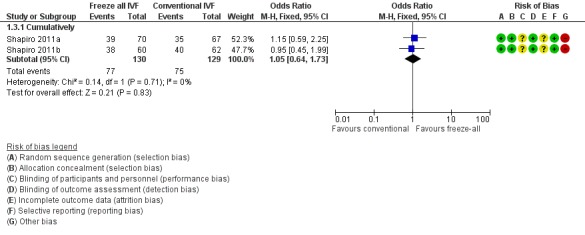
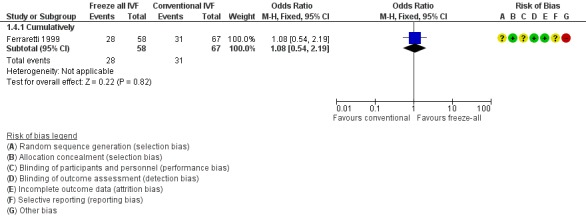
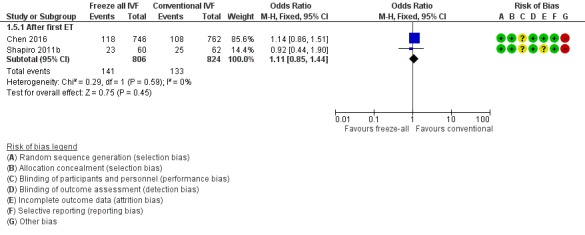
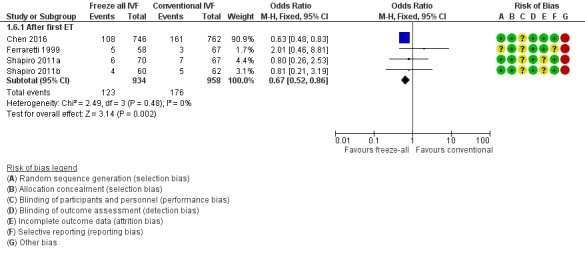
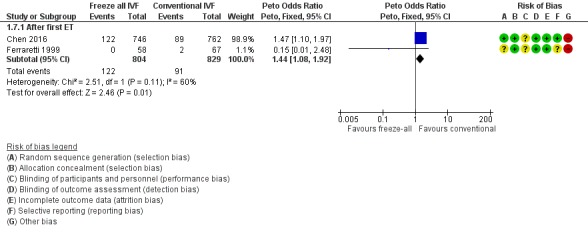
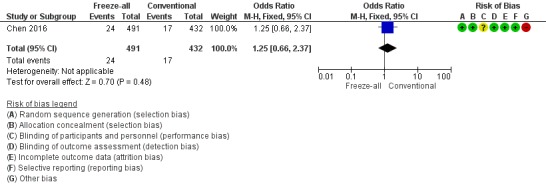
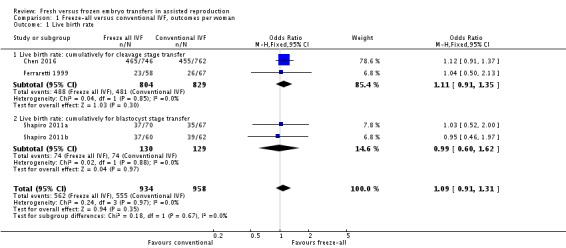
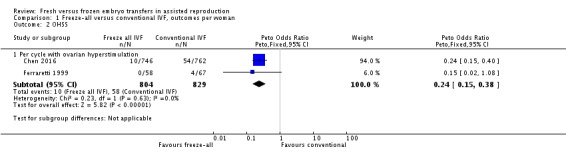
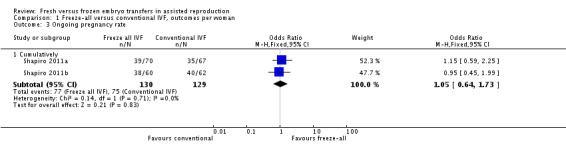
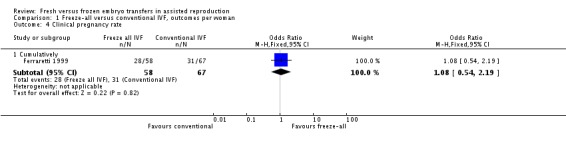
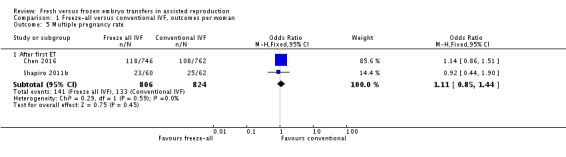
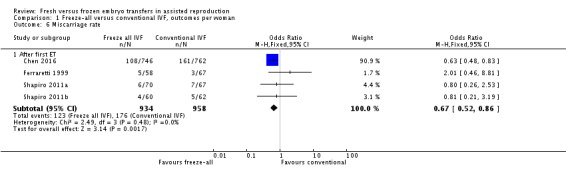
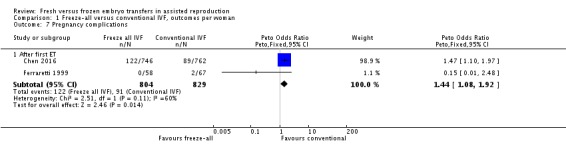
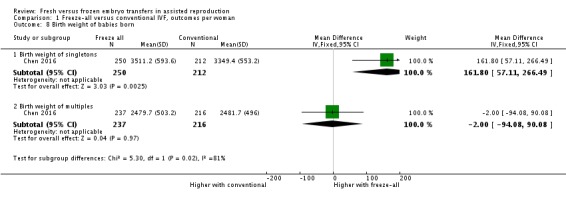
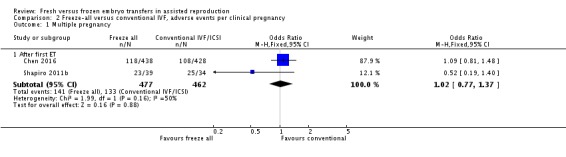
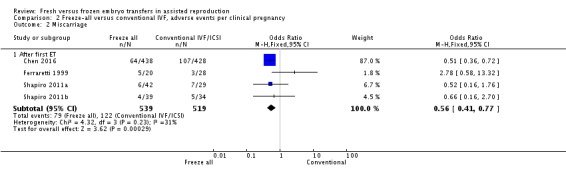
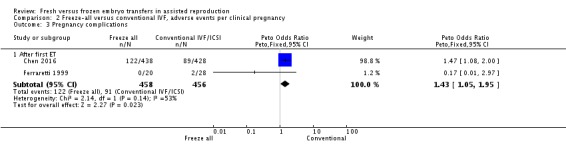
Main results: We included four randomised clinical trials analysing a total of 1892 women comparing a freeze-all strategy with a conventional IVF/ICSI strategy. The evidence was of moderate to low quality due to serious risk of bias and (for some outcomes) serious imprecision. Risk of bias was associated with unclear blinding of investigators for preliminary outcomes of the study, unit of analysis error, and absence of adequate study termination rules.There was no clear evidence of a difference in cumulative live birth rate between the freeze-all strategy and the conventional IVF/ICSI strategy (odds ratio (OR) 1.09, 95% confidence interval (CI) 0.91 to 1.31; 4 trials; 1892 women; I2 = 0%; moderate-quality evidence). This suggests that if the cumulative live birth rate is 58% following a conventional IVF/ICSI strategy, the rate following a freeze-all strategy would be between 56% and 65%.The prevalence of OHSS was lower after the freeze-all strategy compared to the conventional IVF/ICSI strategy (OR 0.24, 95% CI 0.15 to 0.38; 2 trials; 1633 women; I2 = 0%; low-quality evidence). This suggests that if the OHSS rate is 7% following a conventional IVF/ICSI strategy, the rate following a freeze-all strategy would be between 1% and 3%.The freeze-all strategy was associated with fewer miscarriages (OR 0.67, 95% CI 0.52 to 0.86; 4 trials; 1892 women; I2 = 0%; low-quality evidence) and a higher rate of pregnancy complications (OR 1.44, 95% CI 1.08 to 1.92; 2 trials; 1633 women; low-quality evidence). There was no difference in multiple pregnancies per woman after the first transfer (OR 1.11, 95% CI 0.85 to 1.44; 2 trials; 1630 women; low-quality evidence), and no data were reported for time to pregnancy.
Authors' conclusions: We found moderate-quality evidence showing that one strategy is not superior to the other in terms of cumulative live birth rates. Time to pregnancy was not reported, but it can be assumed to be shorter using a conventional IVF/ICSI strategy in the case of similar cumulative live birth rates, as embryo transfer is delayed in a freeze-all strategy. Low-quality evidence suggests that not performing a fresh transfer lowers the OHSS risk for women at risk of OHSS.
Conflict of interest statement
Kai Mee Wong: none known Madelon van Wely: none known Femke Mol: none known Sjoerd Repping: none known Sebastiaan Mastenbroek is principal investigator of one of the ongoing studies.
Figures
References
References to studies included in this review
-
- Chen ZJ, Shi Y, Sun Y, Zhang B, Liang X, Cao Y, et al. Fresh versus frozen embryos for infertility in the polycystic ovary syndrome. New England Journal of Medicine 2016;375(6):523‐33. - PubMed
-
- Ferraretti AP, Gianaroli L, Magli C, Fortini D, Selman HA, Feliciani E. Elective cryopreservation of all pronucleate embryos in women at risk of ovarian hyperstimulation syndrome: efficiency and safety. Human Reproduction 1999;14:1457‐60. [DOI: 10.1093/humrep/14.6.1457; PMID: 10357958 ] - DOI - PubMed
-
- Shapiro BS, Daneshmand ST, Garner FC, Aguirre M, Hudson C, Thomas S. Evidence of impaired endometrial receptivity after ovarian stimulation for in vitro fertilization: A prospective randomized trial comparing fresh and frozen‐thawed embryo transfer in normal responders. Fertility and Sterility 2011;96:344‐8. [DOI: 10.1016/j.fertnstert.2011.05.050; PMID: 21737072 ] - DOI - PubMed
-
- Shapiro BS, Daneshmand ST, Garner FC, Aguirre M, Hudson C, Thomas S. Evidence of impaired endometrial receptivity after ovarian stimulation for in vitro fertilization: A prospective randomized trial comparing fresh and frozen‐thawed embryo transfers in high responders. Fertility and Sterility 2011;96:516‐8. [DOI: 10.1016/j.fertnstert.2011.02.059; PMID: 21737071 ] - DOI - PubMed
References to studies excluded from this review
-
- Aflatoonian A, Oskouian H, Ahmadi S, Oskouian L. Can fresh embryo transfers be replaced by cryopreserved‐thawed embryo transfers in assisted reproductive cycles? A randomized controlled trial. Journal of Assisted Reproduction and Genetics 2010;27:357‐63. [DOI: 10.1007/s10815-010-9412-9; PMID: 20373015 ] - DOI - PMC - PubMed
- Editor and the ASRM Publications Committee. Retraction note to: Can fresh embryo transfers be replaced by cryopreserved‐thawed embryo transfers in assisted reproductive cycles? A randomized controlled trial. Journal of Assisted Reproduction and Genetics 2013;30(9):1245. [DOI: 10.1007; PMID: 23975193 ] - PMC - PubMed
-
- Boostanfar R, Gates D, Guan Y, Gordon K, McCrary Sisk C, Stegmann B. Efficacy and safety of frozen‐thawed embryo transfer in women aged 35 to 42 years from the PURSUE randomized clinical trial. Fertility and Sterility 2016;106(2):300‐5. - PubMed
-
- Yang S, Pang T, Li R, Yang R, Zhen X, Chen X, et al. The individualized choice of embryo transfer timing for patients with elevated serum progesterone level on the HCG day in IVF/ICSI cycles: a prospective randomized clinical study. Gynecological Endocrinology: the official journal of the International Society of Gynecological Endocrinology 2015;31(5):355‐8. [PUBMED: 25558791] - PubMed
References to studies awaiting assessment
References to ongoing studies
-
- ACTRN12612000422820. A randomised controlled trial to determine the effect of elective embryo cryopreservation and subsequent transfer in a natural menstrual cycle on clinical pregnancy rates in infertile females. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=362361 (first received 11 April 2012).
-
- ACTRN12616000643471. Fresh vs. elective frozen embryo transfer after IVF: a randomised controlled trial. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=370373 (first received 24 March 2016).
-
- ISRCTN61225414. Freezing of embryos in assisted conception: a randomised controlled trial evaluating the clinical and cost‐effectiveness of a policy of freezing embryos followed by thawed frozen embryo transfer, compared with a policy of fresh embryo transfer in women undergoing in‐vitro fertilization. www.isrctn.com/ISRCTN61225414 (first received 24 December 2015). - PMC - PubMed
-
- NCT02000349. Comparison of frozen‐thawed embryo transfers and fresh embryo transfers with whole chromosome analysis using next generation sequencing. clinicaltrials.gov/ct2/show/NCT02000349 (first received 19 September 2013).
-
- NCT02133950. Efficacy study of segmentation of PGD treatment. clinicaltrials.gov/ct2/show/NCT02133950 (first received 6 May 2014).
Additional references
-
- Bourgain C, Devroey P. The endometrium in stimulated cycles for IVF. Human Reproduction Update 2003;9:515‐22. - PubMed
-
- Centers for Disease Control and Prevention. Assisted Reproductive Technology Report; 2011. www.cdc.gov/art/ART2011/section5.htm (accessed 25 April 2014).
-
- European Society of Human Reproduction and Embryology (ESHRE). ART Fact Sheet; 2010. www.eshre.eu/ESHRE/English/Guidelines‐Legal/ART‐fact‐sheet/page.aspx/1061 (accessed 25 April 2014).
-
- Ferraretti AP, Magli C, Feliciani E, Montanaro N, Gianaroli L. Relationship of timing of agonist administration in the cycle phase to the ovarian response to gonadotropins in the long down‐regulation protocols for assisted reproductive technologies. Fertility and Sterility 1996;65(1):114‐21. - PubMed
-
- McMaster University. GRADEpro GDT. Version accessed XXX. Hamilton (ON): GRADE Working Group: McMaster University, 2014.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical