

Neuropathological diagnoses and clinical correlates in older adults in Brazil: A cross-sectional study
- PMID: 28350821
- PMCID: PMC5369698
- DOI: 10.1371/journal.pmed.1002267
Neuropathological diagnoses and clinical correlates in older adults in Brazil: A cross-sectional study
Abstract
Background: Clinicopathological studies are important in determining the brain lesions underlying dementia. Although almost 60% of individuals with dementia live in developing countries, few clinicopathological studies focus on these individuals. We investigated the frequency of neurodegenerative and vascular-related neuropathological lesions in 1,092 Brazilian admixed older adults, their correlation with cognitive and neuropsychiatric symptoms, and the accuracy of dementia subtype diagnosis.
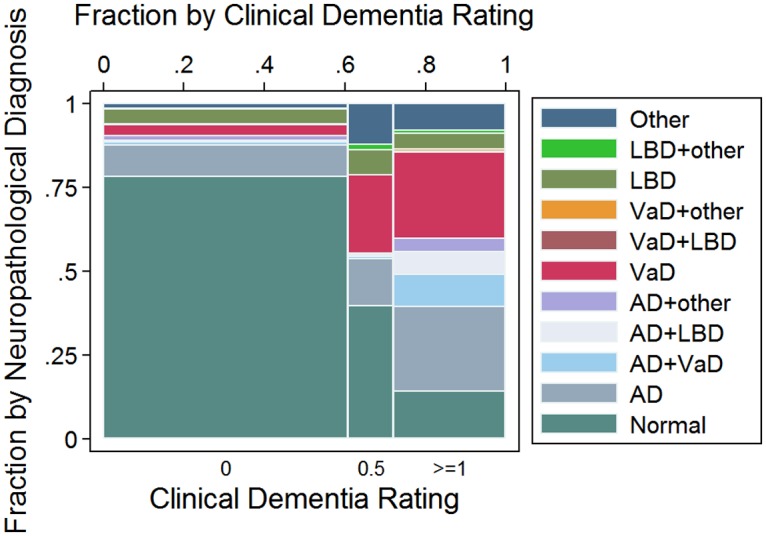
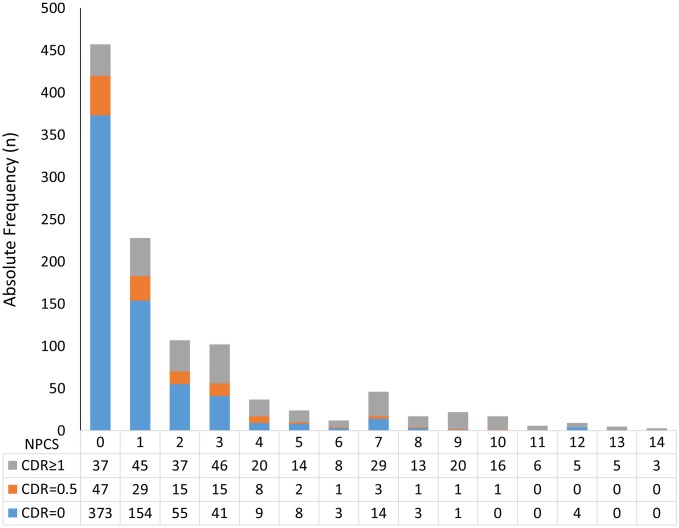
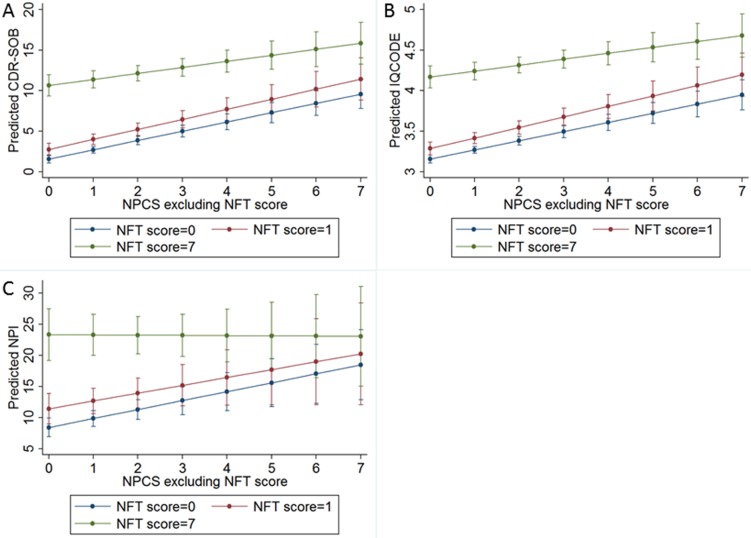
Methods and findings: In this cross-sectional study, we describe clinical and neuropathological variables related to cognitive impairment in 1,092 participants (mean age = 74 y, 49% male, 69% white, and mean education = 4 y). Cognitive function was investigated using the Clinical Dementia Rating (CDR) and the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE); neuropsychiatric symptoms were evaluated using the Neuropsychiatric Inventory (NPI). Associations between neuropathological lesions and cognitive impairment were investigated using ordinal logistic regression. We developed a neuropathological comorbidity (NPC) score and compared it to CDR, IQCODE, and NPI scores. We also described and compared the frequency of neuropathological diagnosis to clinical diagnosis of dementia subtype. Forty-four percent of the sample met criteria for neuropathological diagnosis. Among these participants, 50% had neuropathological diagnoses of Alzheimer disease (AD), and 35% of vascular dementia (VaD). Neurofibrillary tangles (NFTs), hippocampal sclerosis, lacunar infarcts, hyaline atherosclerosis, siderocalcinosis, and Lewy body disease were independently associated with cognitive impairment. Higher NPC scores were associated with worse scores in the CDR sum of boxes (β = 1.33, 95% CI 1.20-1.46), IQCODE (β = 0.14, 95% CI 0.13-0.16), and NPI (β = 1.74, 95% CI = 1.33-2.16). Compared to neuropathological diagnoses, clinical diagnosis had high sensitivity to AD and high specificity to dementia with Lewy body/Parkinson dementia. The major limitation of our study is the lack of clinical follow-up of participants during life.
Conclusions: NFT deposition, vascular lesions, and high NPC scorewere associated with cognitive impairment in a unique Brazilian sample with low education. Our results confirm the high prevalence of neuropathological diagnosis in older adults and the mismatch between clinical and neuropathological diagnoses.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Cairns NJ, Bigio EH, Mackenzie IR, Neumann M, Lee VM, Hatanpaa KJ, et al. Neuropathologic diagnostic and nosologic criteria for frontotemporal lobar degeneration: consensus of the Consortium for Frontotemporal Lobar Degeneration. Acta Neuropathol. 2007;114:5–22. 10.1007/s00401-007-0237-2 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
