

Task-shifting alcohol interventions for HIV+ persons in Kenya: a cost-benefit analysis
- PMID: 28351364
- PMCID: PMC5371255
- DOI: 10.1186/s12913-017-2169-4
Task-shifting alcohol interventions for HIV+ persons in Kenya: a cost-benefit analysis
Abstract
Background: Among HIV+ patients, alcohol use is a highly prevalent risk factor for both HIV transmission and poor adherence to HIV treatment. The large-scale implementation of effective interventions for treating alcohol problems remains a challenge in low-income countries with generalized HIV epidemics. It is essential to consider an intervention's cost-effectiveness in dollars-per-health-outcome, and the long-term economic impact -or "return on investment" in monetary terms.
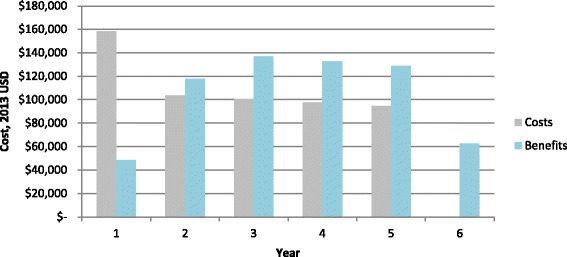
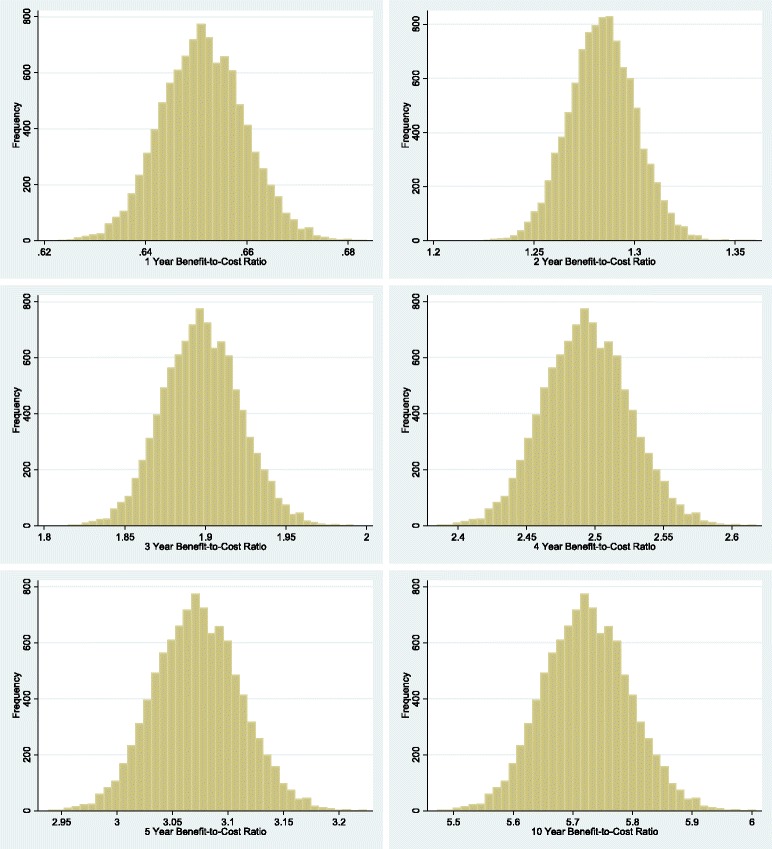
Methods: We conducted a cost-benefit analysis, measuring economic return on investment, of a task-shifted cognitive-behavioral therapy (CBT) intervention delivered by paraprofessionals to reduce alcohol use in a modeled cohort of 13,440 outpatients in Kenya. In our base-case, we estimated the costs and economic benefits from a societal perspective across a six-year time horizon, with a 3% annual discount rate. Costs included all costs associated with training and administering task-shifted CBT therapy. Benefits included the economic impact of lowered HIV incidence as well as the improvements in household and labor-force productivity. We conducted univariate and multivariate probabilistic sensitivity analyses to test the robustness of our results.
Results: Under the base case, total costs for CBT rollout was $554,000, the value of benefits were $628,000, and the benefit-to-cost ratio was 1.13. Sensitivity analyses showed that under most assumptions, the benefit-to-cost ratio remained above unity indicating that the intervention was cost-saving (i.e., had positive return on investment). The duration of the treatment effect most effected the results in sensitivity analyses.
Conclusions: CBT can be effectively and economically task-shifted to paraprofessionals in Kenya. The intervention can generate not only reductions in morbidity and mortality, but also economic savings for the health system in the medium and long term. The findings have implications for other countries with generalized HIV epidemics, high prevalence of alcohol consumption, and shortages of mental health professionals.
Trial registration: This paper uses data derived from "Cognitive Behavioral Treatment to Reduce Alcohol Use Among HIV-Infected Kenyans (KHBS)" with ClinicalTrials.gov registration NCT00792519 on 11/17/2008; and preliminary data from "A Stage 2 Cognitive-behavioral Trial: Reduce Alcohol First in Kenya Intervention" ( NCT01503255 , registered on 12/16/2011).
Keywords: AIDS; Alcohol; CBT; Cognitive-behavioral-therapy; Cost-benefit-analysis; HIV; Kenya; Sub-Saharan Africa; Task-shifting.
Figures

References
-
- WHO . Global Status Report on Alcohol and Health 2014. Geneva: World Health Organization (WHO); 2014.
-
- Bass JK, Bornemann TH, Burkey M, Chehil S, Chen L, Copeland JR, Eaton WW, Ganju V, Hayward E, Hock RS, et al. A United Nations General Assembly Special Session for mental, neurological, and substance use disorders: the time has come. PLoS Med. 2012;9(1) doi: 10.1371/journal.pmed.1001159. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
