

Comparing nonpharmaceutical interventions for containing emerging epidemics
- PMID: 28351976
- PMCID: PMC5393248
- DOI: 10.1073/pnas.1616438114
Comparing nonpharmaceutical interventions for containing emerging epidemics
Abstract
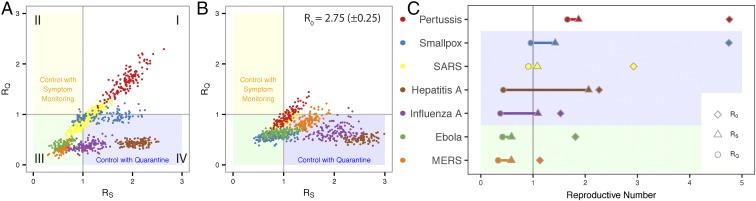
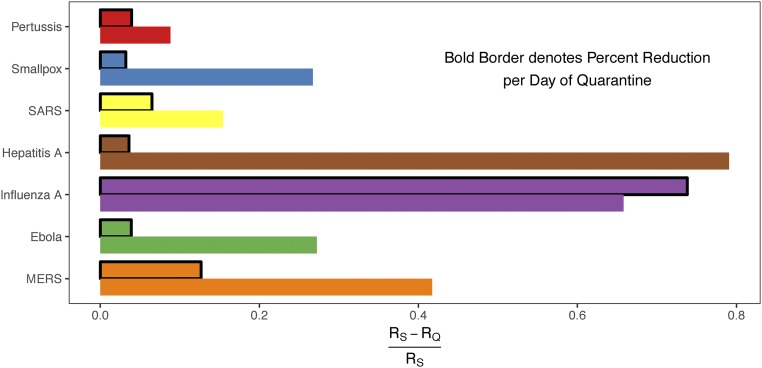
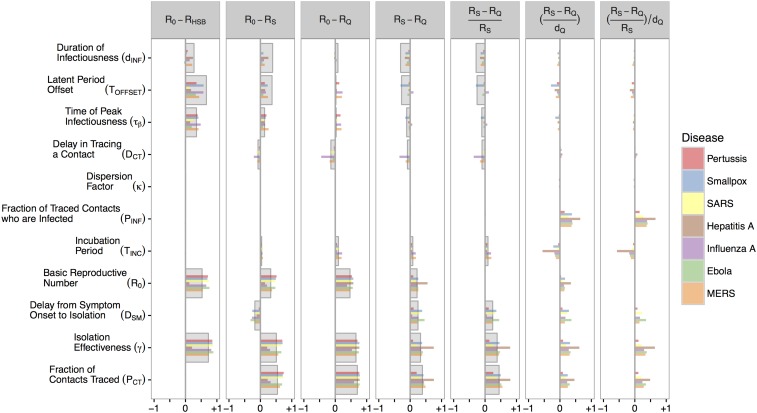
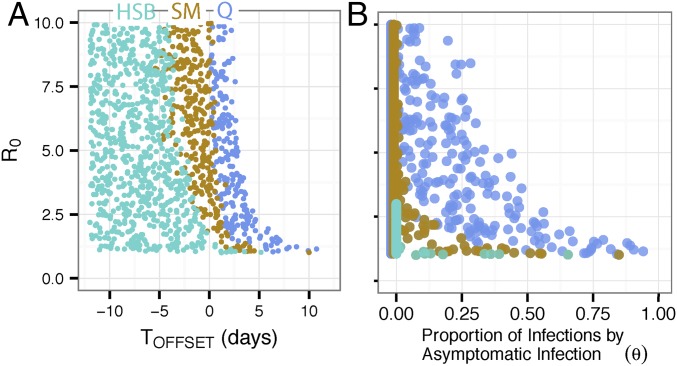
Strategies for containing an emerging infectious disease outbreak must be nonpharmaceutical when drugs or vaccines for the pathogen do not yet exist or are unavailable. The success of these nonpharmaceutical strategies will depend on not only the effectiveness of isolation measures but also the epidemiological characteristics of the infection. However, there is currently no systematic framework to assess the relationship between different containment strategies and the natural history and epidemiological dynamics of the pathogen. Here, we compare the effectiveness of quarantine and symptom monitoring, implemented via contact tracing, in controlling epidemics using an agent-based branching model. We examine the relationship between epidemic containment and the disease dynamics of symptoms and infectiousness for seven case-study diseases with diverse natural histories, including Ebola, influenza A, and severe acute respiratory syndrome (SARS). We show that the comparative effectiveness of symptom monitoring and quarantine depends critically on the natural history of the infectious disease, its inherent transmissibility, and the intervention feasibility in the particular healthcare setting. The benefit of quarantine over symptom monitoring is generally maximized for fast-course diseases, but we show the conditions under which symptom monitoring alone can control certain outbreaks. This quantitative framework can guide policymakers on how best to use nonpharmaceutical interventions and prioritize research during an outbreak of an emerging pathogen.
Keywords: active symptom monitoring; contact tracing; epidemiology; infectious disease dynamics; quarantine.
Conflict of interest statement
The authors declare no conflict of interest.
Figures





References
-
- Barbera J, et al. Large-scale quarantine following biological terrorism in the United States: Scientific examination, logistic and legal limits, and possible consequences. JAMA. 2001;286:2711–2717. - PubMed
-
- American Civil Liberties Union, Yale Global Health Justice Partnership 2015 Fear, Politics, and Ebola. How Quarantines Hurt the Fight Against Ebola and Violate the Constitution. Available at https://www.aclu.org/sites/default/files/field_document/aclu-ebolareport.... Accessed March 10, 2017.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
