

Priming is key to effective incorporation of image-guided thermal ablation into immunotherapy protocols
- PMID: 28352658
- PMCID: PMC5358490
- DOI: 10.1172/jci.insight.90521
Priming is key to effective incorporation of image-guided thermal ablation into immunotherapy protocols
Abstract
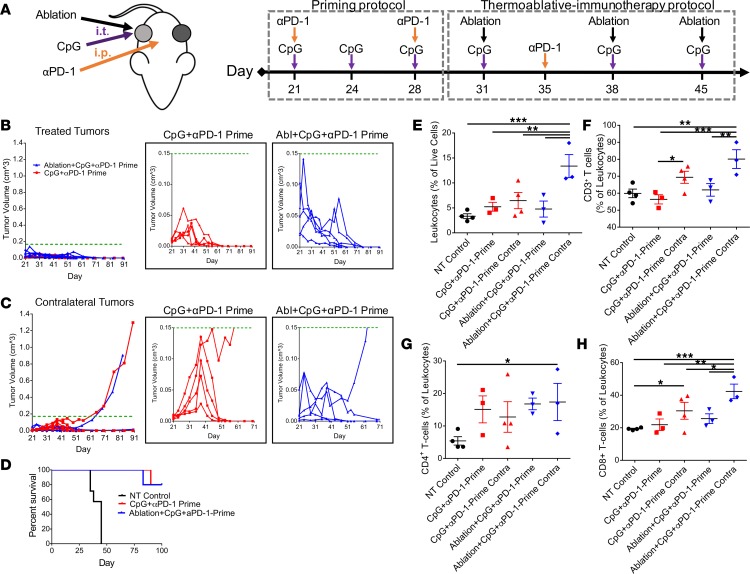
Focal therapies play an important role in the treatment of cancers where palliation is desired, local control is needed, or surgical resection is not feasible. Pairing immunotherapy with such focal treatments is particularly attractive; however, there is emerging evidence that focal therapy can have a positive or negative impact on the efficacy of immunotherapy. Thermal ablation is an appealing modality to pair with such protocols, as tumors can be rapidly debulked (cell death occurring within minutes to hours), tumor antigens can be released locally, and treatment can be conducted and repeated without the concerns of radiation-based therapies. In a syngeneic model of epithelial cancer, we found that 7 days of immunotherapy (TLR9 agonist and checkpoint blockade), prior to thermal ablation, reduced macrophages and myeloid-derived suppressor cells and enhanced IFN-γ-producing CD8+ T cells, the M1 macrophage fraction, and PD-L1 expression on CD45+ cells. Continued treatment with immunotherapy alone or with immunotherapy combined with ablation (primed ablation) then resulted in a complete response in 80% of treated mice at day 90, and primed ablation expanded CD8+ T cells as compared with all control groups. When the tumor burden was increased by implantation of 3 orthotopic tumors, successive primed ablation of 2 discrete lesions resulted in survival of 60% of treated mice as compared with 25% of mice treated with immunotherapy alone. Alternatively, when immunotherapy was begun immediately after thermal ablation, the abscopal effect was diminished and none of the mice within the cohort exhibited a complete response. In summary, we found that immunotherapy begun before ablation can be curative and can enhance efficacy in the presence of a high tumor burden. Two mechanisms have potential to impact the efficacy of immunotherapy when begun immediately after thermal ablation: mechanical changes in the tumor microenvironment and inflammatory-mediated changes in immune phenotype.
Conflict of interest statement
Conflict of interest: The authors have declared that no conflict of interest exists.
Figures






References
-
- Nguyen LT, Ohashi PS. Clinical blockade of PD1 and LAG3--potential mechanisms of action. Nat Rev Immunol. 2015;15(1):45–56. - PubMed
-
- Nowak AK, Robinson BW, Lake RA. Synergy between chemotherapy and immunotherapy in the treatment of established murine solid tumors. Cancer Res. 2003;63(15):4490–4496. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
