

Pulmonary arterovenous malformation causing hemothorax in a pregnant woman without Osler-Weber-Rendu syndrome
- PMID: 28352753
- PMCID: PMC5368882
- DOI: 10.1515/med-2015-0093
Pulmonary arterovenous malformation causing hemothorax in a pregnant woman without Osler-Weber-Rendu syndrome
Abstract
Pulmonary arteriovenous malformations (PAVMs), although most commonly congenital, are usually detected later in life.
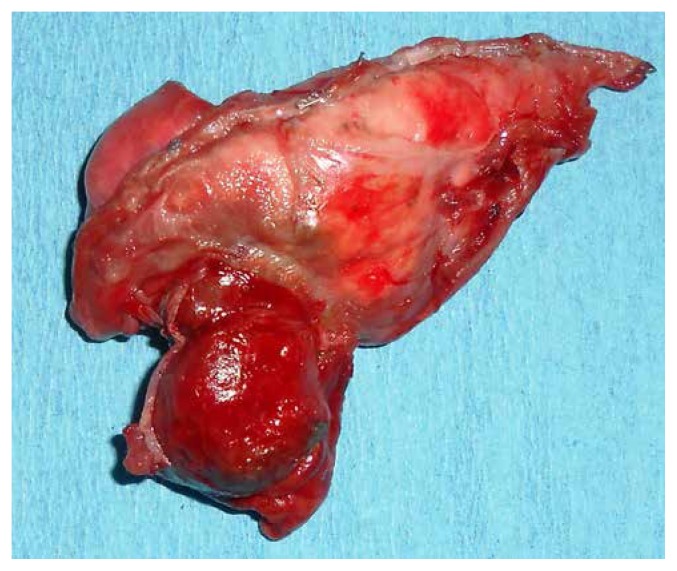
Case report: We present a case of a 19-year-old woman with no previous history of AVM or telangiectasia, who presented dyspnea and hypoxia by massive left hemothorax in the 34th week of gestation. After emergent cesarean delivery, a chest computed tomography (CT) with i.v. contrast showed a likely 3 cm area of active contrast in left lower lung. Chest tube placement revealed about 2 liters of blood. The patient was subsequently found to have pulmonary AVM. A successful embolisation of AVM followed by lung atipic resection involving AVM and decortication for lung re-expansion were the treatments provided.
Conclusions: Women with known pulmonary AVM should be maximally treated prior to becoming pregnant, and the physician should be alert to complications of pulmonary AVM during pregnancy.
Keywords: Osler-Weber-Rendu syndrome; Pulmonary arteriovenous malformations; pregnant woman.
Figures





Similar articles
-
Pulmonary Arteriovenous Malformation (AVM) Causing Tension Hemothorax in a Pregnant Woman Requiring Emergent Cesarean Delivery.Pulm Med. 2011;2011:865195. doi: 10.1155/2011/865195. Epub 2011 Jun 2. Pulm Med. 2011. PMID: 21660210 Free PMC article.
-
Rendu-Osler-Weber syndrome presenting with pulmonary arteriovenous fistula.Australas Radiol. 2005 Jun;49(3):242-5. doi: 10.1111/j.1440-1673.2005.01422.x. Australas Radiol. 2005. PMID: 15932469
-
Pulmonary arteriovenous malformation of Osler-Weber-Rendu syndrome diagnosed by endobronchial ultrasound.Respirology. 2007 Mar;12(2):295-8. doi: 10.1111/j.1440-1843.2006.01025.x. Respirology. 2007. PMID: 17298467
-
Pulmonary vascular manifestations of hereditary hemorrhagic telangiectasia (rendu-osler disease).Respiration. 2007;74(4):361-78. doi: 10.1159/000103205. Respiration. 2007. PMID: 17641482 Review.
-
[Embolotherapy of recanalized symptomatic pulmonary arteriovenous malformations in a patient with Rendu-Osler-Weber syndrome: a case report and review of literature].Przegl Lek. 2012;69(7):320-5. Przegl Lek. 2012. PMID: 23276025 Review. Polish.
Cited by
-
Pulmonary Arteriovenous Malformations (PAVMs) and Pregnancy: A Rare Case of Hemothorax and Review of the Literature.Case Rep Obstet Gynecol. 2019 Apr 28;2019:8165791. doi: 10.1155/2019/8165791. eCollection 2019. Case Rep Obstet Gynecol. 2019. PMID: 31183230 Free PMC article.
-
Attention to pulmonary arteriovenous fistula in a case of transient hypoxemia and cerebral infarction during pregnancy: a case report and literature review.BMC Pregnancy Childbirth. 2023 Aug 31;23(1):626. doi: 10.1186/s12884-023-05946-2. BMC Pregnancy Childbirth. 2023. PMID: 37653522 Free PMC article. Review.
-
Massive hemothorax induced by pulmonary arteriovenous malformation rupture: a case report and literature review.J Cardiothorac Surg. 2024 Jun 21;19(1):342. doi: 10.1186/s13019-024-02867-9. J Cardiothorac Surg. 2024. PMID: 38907280 Free PMC article. Review.
-
Spontaneous Hemothorax by Pulmonary Arteriovenous Malformation during Pregnancy.Thorac Cardiovasc Surg Rep. 2023 Dec 14;12(1):e63-e65. doi: 10.1055/a-2121-7350. eCollection 2023 Jan. Thorac Cardiovasc Surg Rep. 2023. PMID: 38098983 Free PMC article.
-
Lobectomy for Pulmonary Arteriovenous Fistula in a Patient With Rendu-Osler-Weber Disease: A Case Report.In Vivo. 2023 Nov-Dec;37(6):2854-2858. doi: 10.21873/invivo.13402. In Vivo. 2023. PMID: 37905648 Free PMC article.
References
-
- Mason RJ. Murray and Nadel’s textbook of respiratory medicine. 4th ed. Saunders; Philadelphia, USA: 2005. pp. 217–221.
-
- Shovlin CL, Jackson JE, Bamfordetal KB. Primary determinants of ischaemic stroke and cerebral abscess are unrelated to severity of pulmonary arteriovenous malformations in HHT. Thorax. 2008;63:259–266. - PubMed
-
- Gabbe SG. Obstetrics: Normal and Problem Pregnancies. 5th ed chapter 3. Churchill Livingstone; Philadelphia, Pa, USA:
-
- Shovlin CL, Guttmacher AE, Buscarinietal E. Diagnostic criteria for hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber Syndrome) American Journal of Medical Genetics. 2000;91:66–67. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources