

Meningioma recurrence
- PMID: 28352788
- PMCID: PMC5329819
- DOI: 10.1515/med-2016-0032
Meningioma recurrence
Abstract
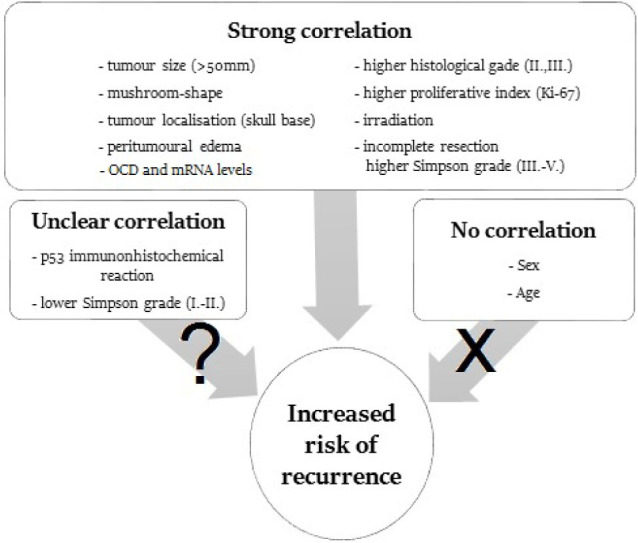
Meningioma accounts for more than 30% of all intracranial tumours. It affects mainly the elderly above the age of 60, at a female:male ratio of 3:2. The prognosis is variable: it is usually favourable with no progression in tumour grade and no recurrence in WHO grade 1 tumours. However, a minority of tumours represent atypical (grade 2) or anaplastic (grade 3) meningiomas; this heterogeneity is also reflected in histopathological appearances. Irrespective of the grade, the size of the tumour and the localisation may have severe, sometimes lethal consequences. Following neurosurgical interventions to remove the tumour, recurrence and progression in WHO grade may occur. Our knowledge on predisposing histomorphological and molecular factors of recurrence is rather limited. These can be classified as I) demographic II) environmental, III) genetic and epigenetic IV) imaging, V) neuropathological, and VI) neurosurgical. In view of the complex background of tumour recurrence, the recognition of often subtle signs of increased risk of recurrence requires close collaboration of experts from several medical specialties. This multidisciplinary approach results in better therapy and fewer complications related to tumour recurrence.
Keywords: Genetics; Immunohistochemistry; Meningioma; Molecular biology; Neuropathology; Pathology; Prognostic factors; Recurrence.
Figures
Similar articles
-
Histopathological prognostic factors of recurrence following definitive therapy for atypical and malignant meningiomas.J Neurosurg. 2018 Apr;128(4):1123-1132. doi: 10.3171/2016.11.JNS16913. Epub 2017 Jun 16. J Neurosurg. 2018. PMID: 28621619
-
Necrosis is a consistent factor to recurrence of meningiomas: should it be a stand-alone grading criterion for grade II meningioma?J Neurooncol. 2018 Apr;137(2):331-336. doi: 10.1007/s11060-017-2721-4. Epub 2017 Dec 21. J Neurooncol. 2018. PMID: 29270884
-
Predictors of early progression of surgically treated atypical meningiomas.Acta Neurochir (Wien). 2018 Sep;160(9):1813-1822. doi: 10.1007/s00701-018-3593-x. Epub 2018 Jun 30. Acta Neurochir (Wien). 2018. PMID: 29961125 Free PMC article.
-
Malignant potential of skull base versus non-skull base meningiomas: clinical series of 1,663 cases.Acta Neurochir (Wien). 2013 Mar;155(3):407-13. doi: 10.1007/s00701-012-1611-y. Epub 2013 Jan 15. Acta Neurochir (Wien). 2013. PMID: 23318687 Review.
-
[Meningioma: management of the most common brain tumour].Praxis (Bern 1994). 2016 Apr 13;105(8):445-51. doi: 10.1024/1661-8157/a002320. Praxis (Bern 1994). 2016. PMID: 27078728 Review. German.
Cited by
-
Alteration of FOXM1 expression and macrophage polarization in refractory meningiomas during long-term follow-up.Transl Cancer Res. 2021 Jan;10(1):553-566. doi: 10.21037/tcr-20-1896. Transl Cancer Res. 2021. PMID: 35116285 Free PMC article.
-
Meningioma Prognostic Tool Based on Correlation of Histopathological Grading and Immunohistochemistry.Oman Med J. 2024 Mar 31;39(2):e608. doi: 10.5001/omj.2024.56. eCollection 2024 Mar. Oman Med J. 2024. PMID: 39055905 Free PMC article.
-
The Sovereignty of Primary Cranial Tumors-Meningiomas: Vetting the Cardinal Epidemiological Features.Med Arch. 2018 Dec;72(6):434-438. doi: 10.5455/medarh.2018.72.434-438. Med Arch. 2018. PMID: 30814776 Free PMC article.
-
Development of a Machine Learning Algorithm for the Prediction of WHO Grade 1 Meningioma Recurrence.Cureus. 2025 Apr 10;17(4):e82033. doi: 10.7759/cureus.82033. eCollection 2025 Apr. Cureus. 2025. PMID: 40352015 Free PMC article.
-
Optimizing the use of Ki-67 proliferative index as a prognostic biomarker in meningiomas using digital analysis.J Neurosurg. 2024 Jul 5;141(6):1644-1654. doi: 10.3171/2024.4.JNS232857. Print 2024 Dec 1. J Neurosurg. 2024. PMID: 38968615
References
-
- Uduma U.F., Emejulu J.C.. Intracranial meningiomas in the present era of modern neuroimaging: diagnostic and management options, with radiological illustrations. Orient J. Med. 2013;25:67–74.
-
- Perry A, Louis D.N., Scheithauer B.W., Budka H, von Deimling, Meningiomas A., Louis DN, Ohgaki H, Wiestler O.D., cavenee W.K. WHO classification of tumours of the central nervous system. IARC; Lyon: 2007. pp. 164–172.
-
- Adegbite A.B., Khan M.I., Paine K.W., Tan L.K.. The recurrence of intracranial meningiomas after surgical treatment. J Neurosurg. 1983;58:51–56. - PubMed
-
- Mahmood A, Qureshi N.H., Malik G.M.. Intracranial meningiomas: analysis of recurrence after surgical treatment. Acta Neurochir (Wien) 1994;126:53–58. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources