

Do Surgeon Expectations Predict Clinically Important Improvements in WOMAC Scores After THA and TKA?
- PMID: 28353050
- PMCID: PMC5539020
- DOI: 10.1007/s11999-017-5331-8
Do Surgeon Expectations Predict Clinically Important Improvements in WOMAC Scores After THA and TKA?
Abstract
Background: Failure of THA or TKA to meet a patient's expectations may result in patient disappointment and litigation. However, there is little evidence to suggest that surgeons can consistently anticipate which patients will benefit from those interventions.
Questions/purposes: To determine the ability of surgeons to identify, in advance of surgery, patients who will benefit from THA or TKA and those who will not, where 'benefit' is defined as a clinically important improvement in a validated patient-reported outcomes score.
Methods: In this prospective study, eight high-volume orthopaedic surgeons completed validated THA and TKA expectations questionnaires (score 0-100, 100 being the highest expectation) as part of preoperative assessment of all their patients scheduled for a THA or TKA and enrolled in the Hospital for Special Surgery institutional registry. Enrolled patients completed the WOMAC preoperatively and at 2 years. Successful outcomes were defined as achieving the minimum clinically important difference (MCID) in WOMAC pain and function subscales. Sensitivity, specificity, and receiver operating characteristic (ROC) curves were used to evaluate the ability of surgeons' expectation scores to identify patients likely to achieve the MCID on the WOMAC scale. Analyses were run separately for patients having THA and TKA. We enrolled 259 patients undergoing THA and 247 undergoing TKA, of whom 77% (n = 200) and 77% (n = 191) completed followup surveys 2 years after their procedures, respectively.
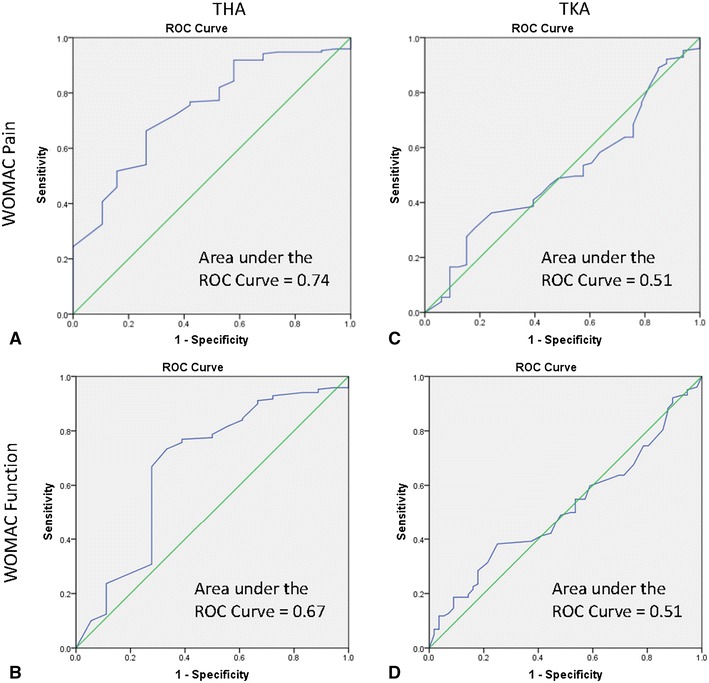
Results: Surgeons' expectation scores effectively anticipated patients who would improve after THA, but they were no better than chance in identifying patients who would achieve the MCID on the WOMAC score 2 years after TKA. For patients having THA, the areas under the ROC curve were 0.67 (95% CI, 0.53-0.82; p = 0.02) and 0.74 (95% CI, 0.63-0.85; p < 0.01) for WOMAC function and pain outcomes, respectively, indicating good accuracy. Sensitivity and specificity were maximized on WOMAC pain and function scores (sensitivity = 0.69, specificity = 0.72, both for pain and function) at an expectations score of 83 or greater of 100. Surgeons' expectations were more accurate for patients who were men, who had a BMI less than 30 kg/m2, who had more than one comorbidity, and who were older than 65 years. For patients having TKA, surgeons' expectation scores were not better than chance for identifying those who would experience a clinically important improvement on the WOMAC scale (area under ROC curve: Function = 0.51, [95% CI, 0.42-0.61], p = 0.78; Pain = 0.51, [95% CI, 0.40-0.61], p = 0.92).
Conclusions: Most patients having THA and TKA achieved the MCID improvement after surgery. However, the inability of surgeons' expectation scores to discriminate accurately between patients who benefit and those who do not among patients scheduled for THA who are young, with no comorbidities, and with elevated BMIs, and among all patients scheduled for TKA, calls for surgeons to spend more time with these patients to fully understand and address their needs and expectations. Using standardized assessment tools to compare surgeons' expectations and those of their patients may help focus the surgeon-patient discussion further, and address patients' expectations more effectively.
Level of evidence: Level II, therapeutic study.
Figures
Comment in
-
Editor's Spotlight/Take 5: Do Surgeon Expectations Predict Clinically Important Improvements in WOMAC Scores After THA and TKA?Clin Orthop Relat Res. 2017 Sep;475(9):2146-2149. doi: 10.1007/s11999-017-5414-6. Epub 2017 Jul 21. Clin Orthop Relat Res. 2017. PMID: 28733952 Free PMC article. No abstract available.
References
-
- Bartholomew DJ. Analysis of Multivariate Social Science Data. 2. Boca Raton, FL: CRC Press; 2008.
-
- Behrend H, Giesinger K, Giesinger JM, Kuster MS. The “forgotten joint” as the ultimate goal in joint arthroplasty: validation of a new patient-reported outcome measure. J Arthroplasty. 2012;27(430–436):e1. - PubMed
-
- Bellamy N. WOMAC Osteoarthritis Index: A User’s Guide. London, Ontario: University of Western Ontario; 1995.
-
- Duivenvoorden T, Vissers MM, Verhaar JA, Busschbach JJ, Gosens T, Bloem RM, Bierma-Zeinstra SM, Reijman M. Anxiety and depressive symptoms before and after total hip and knee arthroplasty: a prospective multicentre study. Osteoarthritis Cartilage. 2013;21:1834–1840. doi: 10.1016/j.joca.2013.08.022. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
