

Effects of photocoagulation on ocular blood flow in patients with severe non-proliferative diabetic retinopathy
- PMID: 28355247
- PMCID: PMC5371365
- DOI: 10.1371/journal.pone.0174427
Effects of photocoagulation on ocular blood flow in patients with severe non-proliferative diabetic retinopathy
Abstract
Purpose: To investigate ocular blood flow and correlations between ocular blood flow and variables in patients with severe non-proliferative diabetic retinopathy (S-NPDR) following panretinal photocoagulation (PRP).
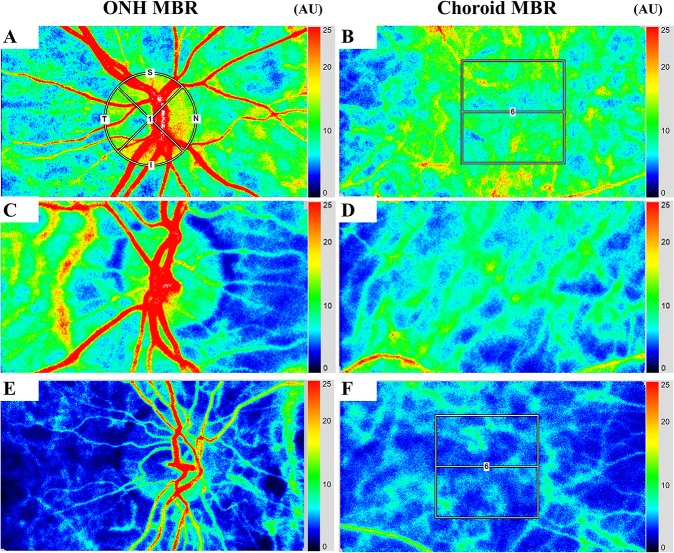
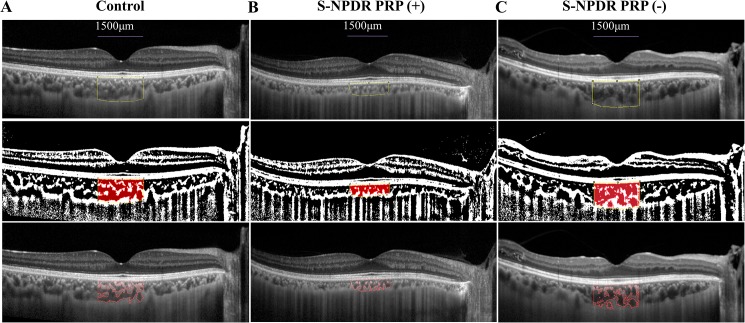
Methods: In this retrospective, cross-sectional study, the blood flow on the optic nerve head (ONH) and choroid was assessed with laser speckle flowgraphy (LSFG) using the mean blur rate (MBR) in 76 eyes of 76 patients with S-NPDR who underwent PRP, 39 eyes of 39 patients with S-NPDR who did not undergo PRP, and 71 eyes of 71 normal subjects. The correlation between MBR and variables, including visual acuity (VA) and choroidal area determined by binarization method, was analyzed.
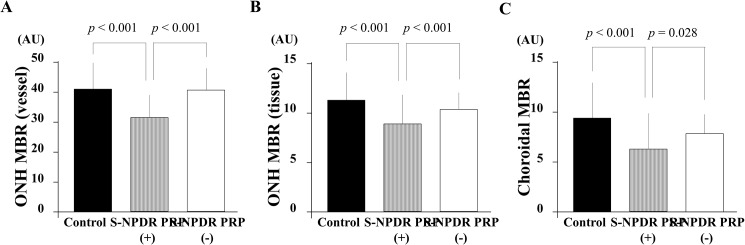
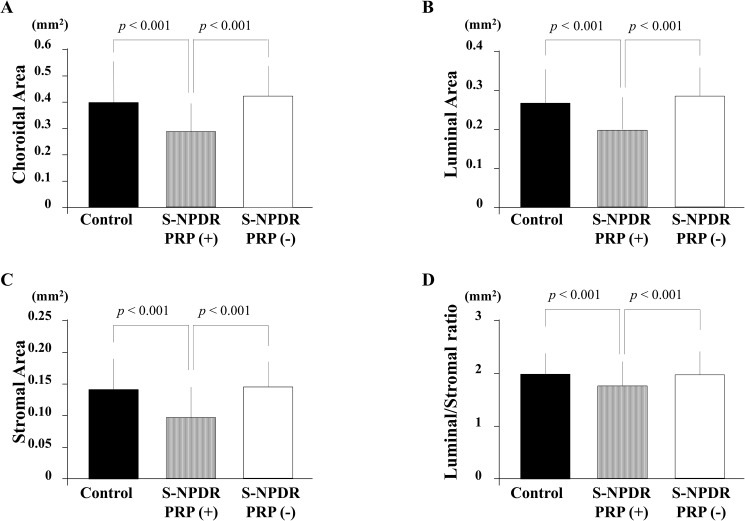
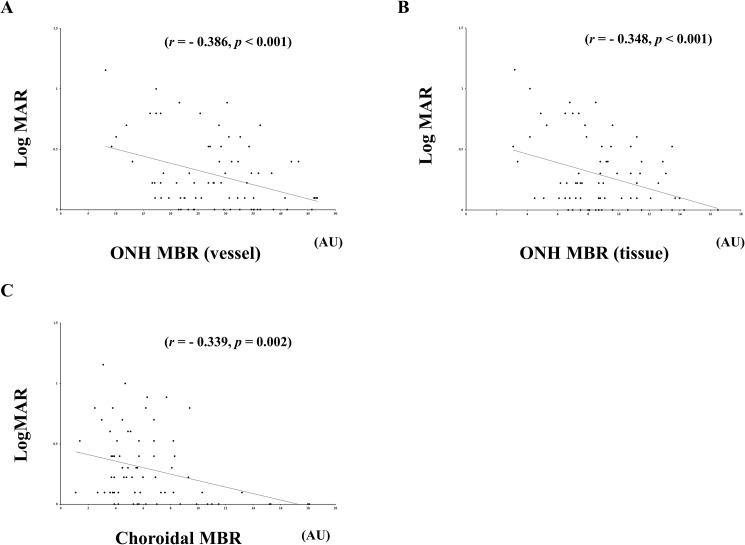
Results: The mean age was 62.9 ± 11.9 years in the S-NPDR with PRP eyes, 55.6 ± 11.4 years in the S-NPDR without PRP eyes, and 60.3 ± 11.1 years in the normal subject eyes. The ONH MBR in vessel and tissue areas and the choroidal MBR were significantly lower in the S-NDR with PRP group than in the other groups (p < 0.001, p < 0.001, and p < 0.001, respectively). The luminal and the stromal areas were significantly smaller in the S-NDR with PRP group than in the other groups (p < 0.001 and p < 0.001, respectively). LogMAR best corrected visual acuity (BCVA) exhibited significant negative correlation with the ONH MBR in vessel (r = -0.386, p < 0.001), tissue (r = -0.348, p < 0.001), and the choroid MBR (r = -0.339, p = 0.002) in the S-NDR with PRP group. Stepwise multiple regression analysis demonstrated that BCVA was a common independent factor associated with the ONH MBR in vessel, tissue, and the choroidal MBR in the S-NDR with PRP group.
Conclusions: ONH and choroid MBR in addition to choroidal component, including the luminal area, were significantly lower in eyes of patients with S-NPDR after PRP compared with no PRP and normal subjects group. This could suggest that the significantly reduced ocular blood flow in PRP-treated S-NPDR eyes correlated with long-term decreased post-PRP luminal area and visual acuity.
Conflict of interest statement
Figures
Similar articles
-
Evaluation of blood flow on optic nerve head after pattern scan and conventional laser panretinal photocoagulation.Medicine (Baltimore). 2019 Jun;98(24):e16062. doi: 10.1097/MD.0000000000016062. Medicine (Baltimore). 2019. PMID: 31192968 Free PMC article. Clinical Trial.
-
Effect of panretinal photocoagulation on retinal oxygen metabolism and ocular blood flow in diabetic retinopathy.Acta Ophthalmol. 2025 Jun;103(4):380-387. doi: 10.1111/aos.17442. Epub 2025 Jan 30. Acta Ophthalmol. 2025. PMID: 39887558
-
Evaluation of retinal blood flow before and after panretinal photocoagulation using pattern scan laser for diabetic retinopathy.Curr Eye Res. 2017 Dec;42(12):1707-1712. doi: 10.1080/02713683.2017.1358373. Epub 2017 Sep 22. Curr Eye Res. 2017. PMID: 28937857
-
[In vivo measurement of ocular circulation with the laser speckle method--development of apparatus and application in ophthalmological research].Nippon Ganka Gakkai Zasshi. 1999 Dec;103(12):871-909. Nippon Ganka Gakkai Zasshi. 1999. PMID: 10643292 Review. Japanese.
-
Choroidal vascular structures in diabetic patients: a meta-analysis.Graefes Arch Clin Exp Ophthalmol. 2021 Dec;259(12):3537-3548. doi: 10.1007/s00417-021-05292-z. Epub 2021 Jul 10. Graefes Arch Clin Exp Ophthalmol. 2021. PMID: 34244824 Review.
Cited by
-
A randomized clinical trial evaluating choroidal blood flow and morphology after conventional and pattern scan laser panretinal photocoagulation.Sci Rep. 2018 Sep 20;8(1):14128. doi: 10.1038/s41598-018-32487-y. Sci Rep. 2018. PMID: 30237467 Free PMC article. Clinical Trial.
-
Retinal Neurovascular Coupling in Diabetes.J Clin Med. 2020 Sep 1;9(9):2829. doi: 10.3390/jcm9092829. J Clin Med. 2020. PMID: 32882896 Free PMC article. Review.
-
Alterations in choroidal vascular parameters following panretinal photocoagulation using enhanced-depth imaging optical coherence tomography in diabetic retinopathy.Graefes Arch Clin Exp Ophthalmol. 2022 Feb;260(2):459-469. doi: 10.1007/s00417-021-05401-y. Epub 2021 Sep 1. Graefes Arch Clin Exp Ophthalmol. 2022. PMID: 34468831
-
Association of Speckle-Based Blood Flow Measurements and Fluorescein Angiography in Infants with Retinopathy of Prematurity.Ophthalmol Sci. 2023 Dec 29;4(4):100463. doi: 10.1016/j.xops.2023.100463. eCollection 2024 Jul-Aug. Ophthalmol Sci. 2023. PMID: 38591050 Free PMC article.
-
Evaluation of blood flow on optic nerve head after pattern scan and conventional laser panretinal photocoagulation.Medicine (Baltimore). 2019 Jun;98(24):e16062. doi: 10.1097/MD.0000000000016062. Medicine (Baltimore). 2019. PMID: 31192968 Free PMC article. Clinical Trial.
References
-
- Preliminary report on effects of photocoagulation therapy. The Diabetic Retinopathy Study Research Group. Am J Ophthalmol. 1976;81(4):383–96. Epub 1976/04/01. - PubMed
-
- Photocoagulation treatment of proliferative diabetic retinopathy. Clinical application of Diabetic Retinopathy Study (DRS) findings, DRS Report Number 8. The Diabetic Retinopathy Study Research Group. Ophthalmology. 1981;88(7):583–600. Epub 1981/07/01. - PubMed
-
- Early photocoagulation for diabetic retinopathy. ETDRS report number 9. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology. 1991;98(5 Suppl):766–85. Epub 1991/05/01. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
