

Dermoscopic Clues for Diagnosing Melanomas That Resemble Seborrheic Keratosis
- PMID: 28355453
- PMCID: PMC5540029
- DOI: 10.1001/jamadermatol.2017.0129
Dermoscopic Clues for Diagnosing Melanomas That Resemble Seborrheic Keratosis
Abstract
Importance: Melanomas that clinically mimic seborrheic keratosis (SK) can delay diagnosis and adequate treatment. However, little is known about the value of dermoscopy in recognizing these difficult-to-diagnose melanomas.
Objective: To describe the dermoscopic features of SK-like melanomas to understand their clinical morphology.
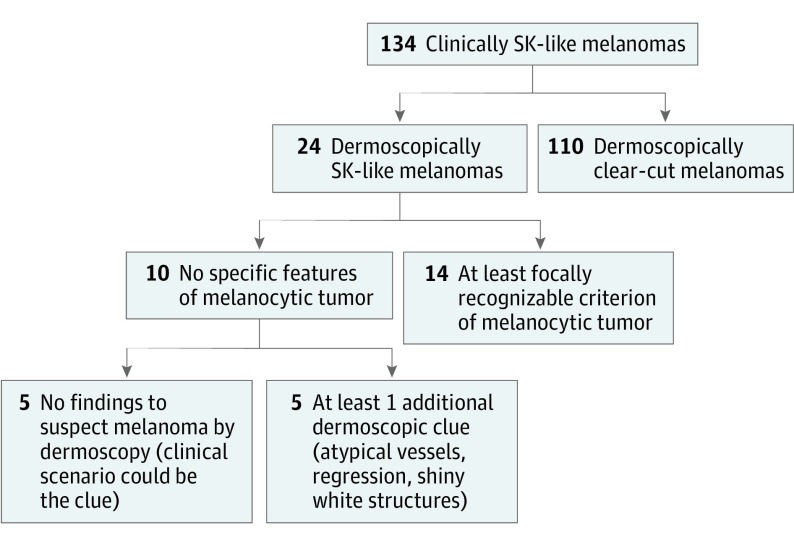
Design, setting, and participants: This observational retrospective study used 134 clinical and dermoscopic images of histopathologically proven melanomas in 134 patients treated in 9 skin cancer centers in Spain, France, Italy, and Austria. Without knowledge that the definite diagnosis for all the lesions was melanoma, 2 dermoscopy-trained observers evaluated the clinical descriptions and 48 dermoscopic features (including all melanocytic and nonmelanocytic criteria) of all 134 images and classified each dermoscopically as SK or not SK. The total dermoscopy score and the 7-point checklist score were assessed. Images of the lesions and patient data were collected from July 15, 2013, through July 31, 2014.
Main outcomes and measures: Frequencies of specific morphologic patterns of (clinically and dermoscopically) SK-like melanomas, patient demographics, and interobserver agreement of criteria were evaluated.
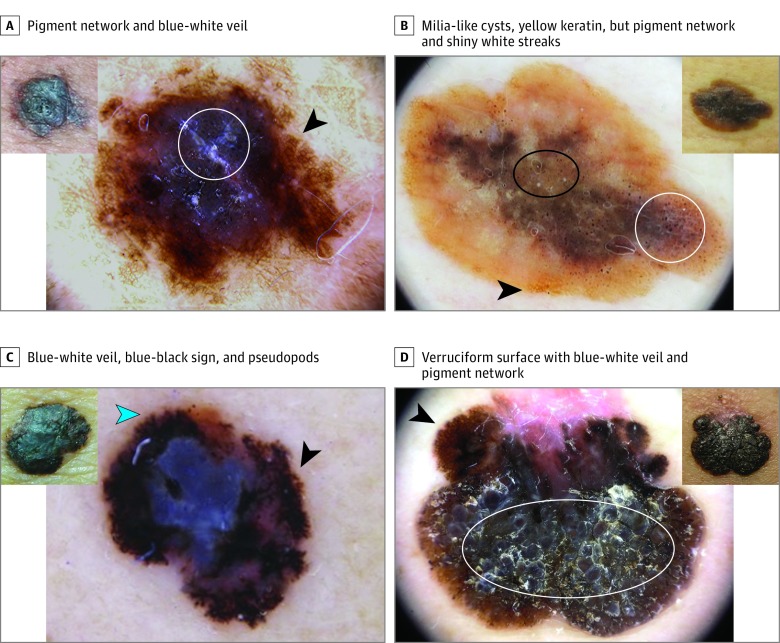
Results: Of the 134 cases collected from 72 men and 61 women, all of whom were white and who had a mean (SD) age of 55.6 (17.5) years, 110 (82.1%) revealed dermoscopic features suggestive of melanoma, including pigment network (74 [55.2%]), blue-white veil (72 [53.7%]), globules and dots (68 [50.7%]), pseudopods or streaks (47 [35.1%]), and blue-black sign (43 [32.3%]). The remaining 24 cases (17.9%) were considered likely SKs, even by dermoscopy. Overall, lesions showed a scaly and hyperkeratotic surface (45 [33.6%]), yellowish keratin (42 [31.3%]), comedo-like openings (41 [30.5%]), and milia-like cysts (30 [22.4%]). The entire sample achieved a mean (SD) total dermoscopy score of 4.7 (1.6) and a 7-point checklist score of 4.4 (2.3), while dermoscopically SK-like melanomas achieved a total dermoscopy score of only 4.2 (1.3) and a 7-point checklist score of 2.0 (1.9), both in the range of benignity. The most helpful criteria in correctly diagnosing SK-like melanomas were the presence of blue-white veil, pseudopods or streaks, and pigment network. Multivariate analysis found only the blue-black sign to be significantly associated with a correct diagnosis, while hyperkeratosis and fissures and ridges were independent risk markers of dermoscopically SK-like melanomas.
Conclusions and relevance: Seborrheic keratosis-like melanomas can be dermoscopically challenging, but the presence of the blue-black sign, pigment network, pseudopods or streaks, and/or blue-white veil, despite the presence of other SK features, allows the correct diagnosis of most of the difficult melanoma cases.
Conflict of interest statement
Figures

Similar articles
-
Dermoscopy Improves the Diagnostic Accuracy of Melanomas Clinically Resembling Seborrheic Keratosis: Cross-Sectional Study of the Ability to Detect Seborrheic Keratosis-Like Melanomas by a Group of Dermatologists with Varying Degrees of Experience.Dermatology. 2017;233(6):471-479. doi: 10.1159/000486851. Epub 2018 Mar 2. Dermatology. 2017. PMID: 29502116
-
The blue globular pattern in dermoscopy.Dermatology. 2013;226(3):260-6. doi: 10.1159/000350257. Epub 2013 Jun 21. Dermatology. 2013. PMID: 23796824
-
Dermoscopy-pathology relationship in seborrheic keratosis.J Dermatol. 2017 May;44(5):518-524. doi: 10.1111/1346-8138.13657. J Dermatol. 2017. PMID: 28447350 Review.
-
Differentiating seborrheic keratosis from melanoma among lesions exhibiting blue-white veil: A retrospective study.J Am Acad Dermatol. 2025 Mar;92(3):480-486. doi: 10.1016/j.jaad.2024.10.070. Epub 2024 Nov 9. J Am Acad Dermatol. 2025. PMID: 39528164
-
Seborrheic keratosis-like melanoma: a diagnostic challenge.Melanoma Res. 2021 Oct 1;31(5):407-412. doi: 10.1097/CMR.0000000000000756. Melanoma Res. 2021. PMID: 34132226 Review.
Cited by
-
Frequency of Publication of Dermoscopic Images in Inter-observer Studies: A Systematic Review.Acta Derm Venereol. 2021 Dec 17;101(12):adv00621. doi: 10.2340/actadv.v101.865. Acta Derm Venereol. 2021. PMID: 34853864 Free PMC article.
-
The potential of x-ray virtual histology in the diagnosis of skin tumors.Skin Res Technol. 2024 Oct;30(10):e13801. doi: 10.1111/srt.13801. Skin Res Technol. 2024. PMID: 39363439 Free PMC article.
-
Polymorphic Vessels-Think About Seborrheic Keratosis.Dermatol Pract Concept. 2020 Oct 26;10(4):e2020090. doi: 10.5826/dpc.1004a90. eCollection 2020 Oct. Dermatol Pract Concept. 2020. PMID: 33150031 Free PMC article. No abstract available.
-
Dermoscopy for Cutaneous Melanoma: Under the Eye of Both the Dermatologist and the Legal Doctor.Dermatol Pract Concept. 2022 Jul 1;12(3):e2022100. doi: 10.5826/dpc.1203a100. eCollection 2022 Jul. Dermatol Pract Concept. 2022. PMID: 36159108 Free PMC article. Review. No abstract available.
-
Clinical spectrum of cutaneous melanoma morphology.J Am Acad Dermatol. 2019 Jan;80(1):178-188.e3. doi: 10.1016/j.jaad.2018.08.028. Epub 2018 Aug 28. J Am Acad Dermatol. 2019. PMID: 30165162 Free PMC article.
References
-
- Izikson L, Sober AJ, Mihm MC Jr, Zembowicz A. Prevalence of melanoma clinically resembling seborrheic keratosis: analysis of 9204 cases. Arch Dermatol. 2002;138(12):1562-1566. - PubMed
-
- Lim C. Seborrhoeic keratoses with associated lesions: a retrospective analysis of 85 lesions. Australas J Dermatol. 2006;47(2):109-113. - PubMed
-
- Braun RP, Rabinovitz HS, Krischer J, et al. . Dermoscopy of pigmented seborrheic keratosis: a morphological study. Arch Dermatol. 2002;138(12):1556-1560. - PubMed
-
- Lin J, Han S, Cui L, et al. . Evaluation of dermoscopic algorithm for seborrhoeic keratosis: a prospective study in 412 patients. J Eur Acad Dermatol Venereol. 2014;28(7):957-962. - PubMed
-
- Kuehnl-Petzoldt C, Berger H, Wiebelt H. Verrucous-keratotic variations of malignant melanoma: a clinicopathological study. Am J Dermatopathol. 1982;4(5):403-410. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
