

Current Treatment Strategies for Intracranial Aneurysms: An Overview
- PMID: 28355880
- PMCID: PMC5724574
- DOI: 10.1177/0003319717700503
Current Treatment Strategies for Intracranial Aneurysms: An Overview
Abstract
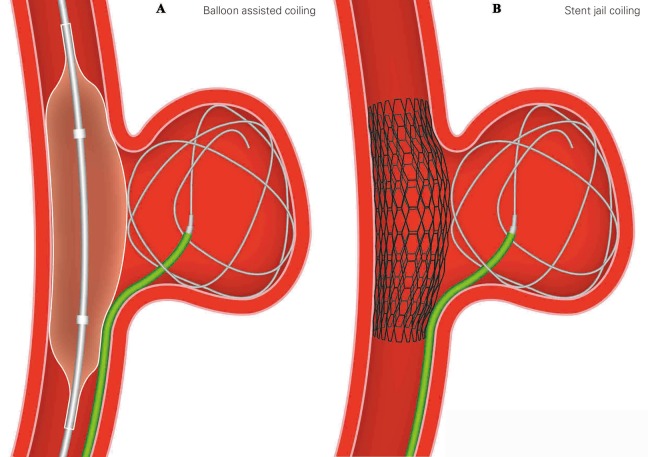
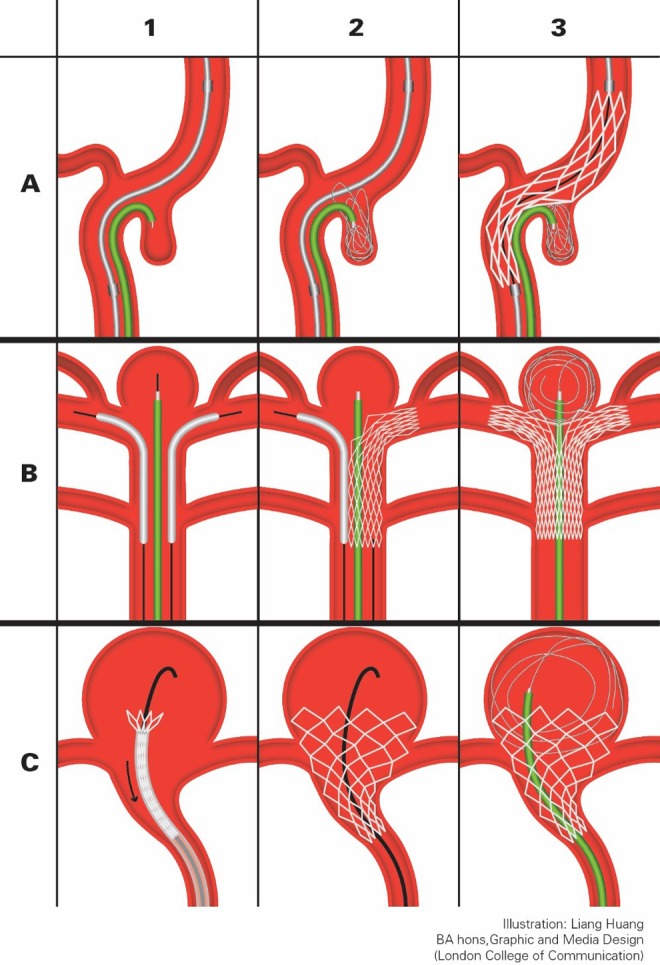
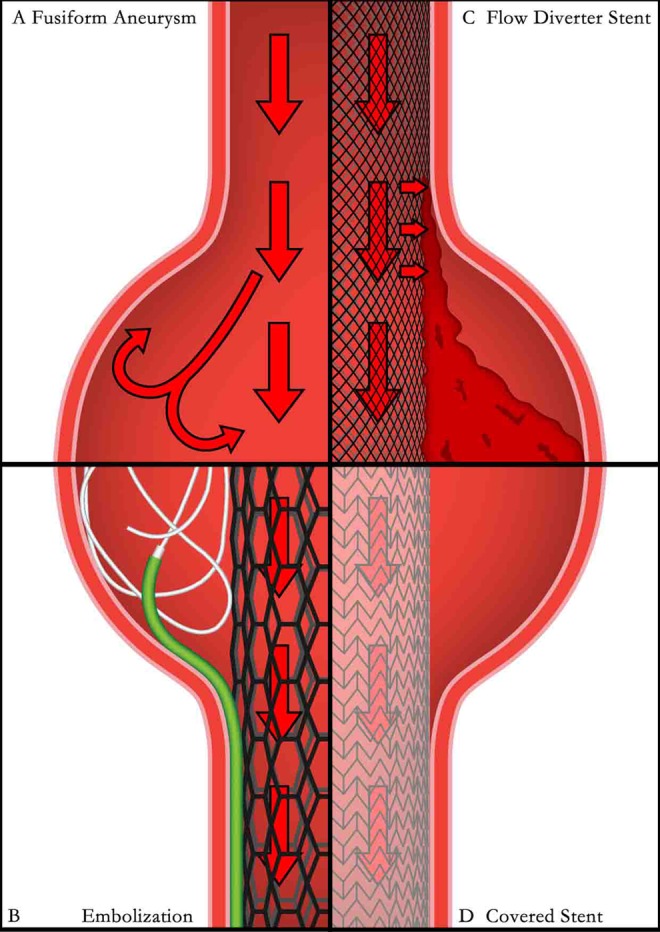
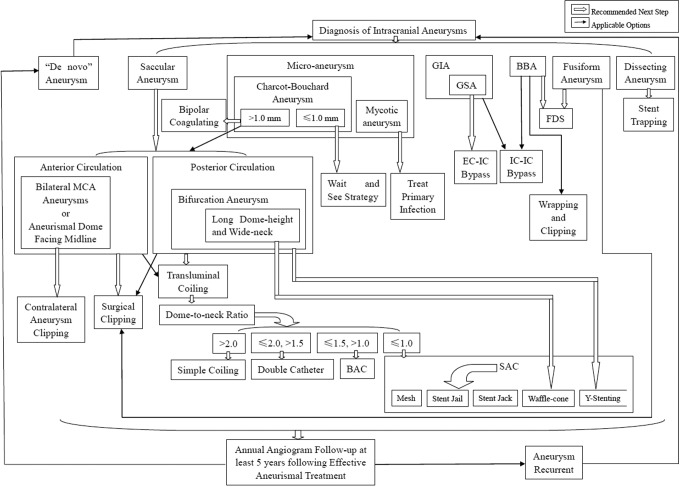
Intracranial aneurysm is a leading cause of stroke. Its treatment has evolved over the past 2 decades. This review summarizes the treatment strategies for intracranial aneurysms from 3 different perspectives: open surgery approach, transluminal treatment approach, and new technologies being used or trialed. We introduce most of the available treatment techniques in detail, including contralateral clipping, wrapping and clipping, double catheters assisting coiling and waffle-cone technique, and so on. Data from major trials such as Analysis of Treatment by Endovascular approach of Non-ruptured Aneurysms (ATENA), Internal Subarachnoid Trial (ISAT), Clinical and Anatomical Results in the Treatment of Ruptured Intracranial Aneurysms (CLARITY), and Barrow Ruptured Aneurysm Trial (BRAT) as well as information from other clinical reports and local experience are reviewed to suggest a clinical pathway for treating different types of intracranial aneurysms. It will be a valuable supplement to the current existing guidelines. We hope it could help assisting real-time decision-making in clinical practices and also encourage advancements in managing the disease.
Keywords: angiography; cerebral revascularization; intracranial aneurysm; intracranial vasospasm; stenting; stroke.
Conflict of interest statement
Figures
Similar articles
-
Treatment of ruptured intracranial aneurysms: implications of the ISAT on clipping versus coiling.Eur J Radiol. 2003 Jun;46(3):172-7. doi: 10.1016/s0720-048x(03)00089-5. Eur J Radiol. 2003. PMID: 12758112 Review.
-
The Barrow Ruptured Aneurysm Trial: 3-year results.J Neurosurg. 2013 Jul;119(1):146-57. doi: 10.3171/2013.3.JNS12683. Epub 2013 Apr 26. J Neurosurg. 2013. PMID: 23621600 Clinical Trial.
-
The durability of endovascular coiling versus neurosurgical clipping of ruptured cerebral aneurysms: 18 year follow-up of the UK cohort of the International Subarachnoid Aneurysm Trial (ISAT).Lancet. 2015 Feb 21;385(9969):691-7. doi: 10.1016/S0140-6736(14)60975-2. Epub 2014 Oct 28. Lancet. 2015. PMID: 25465111 Free PMC article. Clinical Trial.
-
Endovascular therapeutic strategies in ruptured intracranial aneurysms.Eur J Radiol. 2013 Oct;82(10):1646-52. doi: 10.1016/j.ejrad.2013.01.034. Epub 2013 Mar 21. Eur J Radiol. 2013. PMID: 23523515 Review.
-
Neurological outcomes following intraprocedural rerupture during coil embolization of ruptured intracranial aneurysms.J Neurosurg. 2015 Jan;122(1):128-35. doi: 10.3171/2014.9.JNS14616. J Neurosurg. 2015. PMID: 25361491
Cited by
-
Efficacy and safety of eight types Salvia miltiorrhiza injections in the treatment of unstable angina pectoris: A network meta-analysis.Front Pharmacol. 2022 Oct 3;13:972738. doi: 10.3389/fphar.2022.972738. eCollection 2022. Front Pharmacol. 2022. PMID: 36263128 Free PMC article.
-
Periprocedural to 1-year safety and efficacy outcomes with the Pipeline Embolization Device with Shield technology for intracranial aneurysms: a prospective, post-market, multi-center study.J Neurointerv Surg. 2020 Nov;12(11):1107-1112. doi: 10.1136/neurintsurg-2020-015943. Epub 2020 Jun 1. J Neurointerv Surg. 2020. PMID: 32482834 Free PMC article. Clinical Trial.
-
Endovascular treatment of intracranial vertebral artery dissecting aneurysm, a case series study with two years follow up on complications.Heliyon. 2023 Apr 19;9(5):e15568. doi: 10.1016/j.heliyon.2023.e15568. eCollection 2023 May. Heliyon. 2023. PMID: 37153412 Free PMC article.
-
The use of three-dimensional anatomical patient-specific printed models in surgical clipping of intracranial aneurysm: A pilot study.Surg Neurol Int. 2020 Nov 11;11:381. doi: 10.25259/SNI_361_2020. eCollection 2020. Surg Neurol Int. 2020. PMID: 33408915 Free PMC article.
-
The evolution of intracranial aneurysm treatment techniques and future directions.Neurosurg Rev. 2022 Feb;45(1):1-25. doi: 10.1007/s10143-021-01543-z. Epub 2021 Apr 23. Neurosurg Rev. 2022. PMID: 33891216 Free PMC article. Review.
References
-
- Vlak MH, Algra A, Brandenburg R, Rinkel GJ. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: systematic review and meta-analysis. Lancet Neurol. 2011;10(7):626–636. - PubMed
-
- van Gijn J, Kerr RS, Rinkel GJ. Subarachnoid haemorrhage. Lancet. 2007;369(9558):306–318. - PubMed
-
- American Stroke Association. Stroke Statistics. London, UK: Stroke Association; 2013.
-
- Bharatha A, Yeung R, Durant D, et al. Comparison of computed tomography angiography with digital subtraction angiography in the assessment of clipped intracranial aneurysms. J Comput Assist Tomogr. 2010;34(3):440–445. - PubMed
-
- Karasawa H, Matsumoto H, Naito H, Sugiyama K, Ueno J, Kin H. Angiographically unrecognized microaneurysms: intraoperative observation and operative technique. Acta Neurochir (Wien). 1997;139(5):416–419; discussion 419-420. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
