

Calcium oxalate crystal related kidney injury in a patient receiving Roux-en Y hepaticojejunostomy due to gall bladder cancer
- PMID: 28356078
- PMCID: PMC5372328
- DOI: 10.1186/s12882-017-0520-y
Calcium oxalate crystal related kidney injury in a patient receiving Roux-en Y hepaticojejunostomy due to gall bladder cancer
Abstract
Background: Calcium oxalate nephropathy is rare in current practice. It was a common complication during jejunoileal bypass, but much less seen in modern gastric bypass surgery for morbid obesity. The major cause of it is enteric hyperoxaluria.
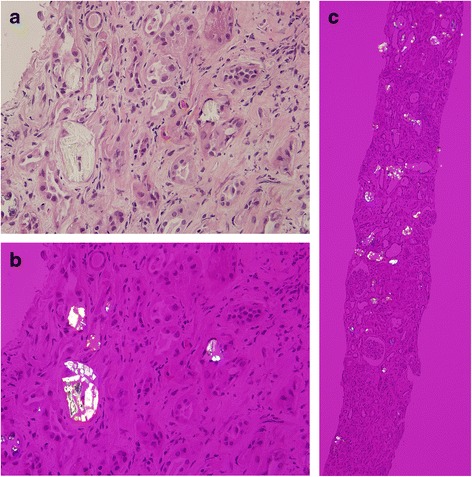
Case presentation: We report on a patient here with acute kidney disease due to calcium oxalate nephropathy, rather than the conditions mentioned above. The male patient received a Roux-en Y hepaticojejunostomy and common bile duct drainage. In addition to enteric hyperoxaluria, chronic kidney disease related metabolic acidosis, chronic diarrhea related volume depletion, a high oxalate and low potassium diet, long term ascorbic acid intake and long term exposure to antibiotics, all predisposed him to having oxalate nephropathy.
Conclusion: This is the first case with such conditions and we recommend that similarly diagnosed patients avoid all these predisposing factors, in order to avoid this rare disease and its undesired outcome.
Keywords: Acute kidney injury; Calcium oxalate; Roux-en Y hepaticojejunostomy.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
