

Adaptive goal setting and financial incentives: a 2 × 2 factorial randomized controlled trial to increase adults' physical activity
- PMID: 28356097
- PMCID: PMC5372290
- DOI: 10.1186/s12889-017-4197-8
Adaptive goal setting and financial incentives: a 2 × 2 factorial randomized controlled trial to increase adults' physical activity
Erratum in
-
Erratum to: Adaptive goal setting and financial incentives: a 2 × 2 factorial randomized controlled trial to increase adults' physical activity.BMC Public Health. 2017 Apr 6;17(1):303. doi: 10.1186/s12889-017-4231-x. BMC Public Health. 2017. PMID: 28385148 Free PMC article. No abstract available.
Abstract
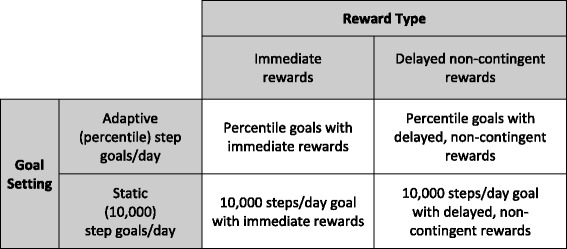
Background: Emerging interventions that rely on and harness variability in behavior to adapt to individual performance over time may outperform interventions that prescribe static goals (e.g., 10,000 steps/day). The purpose of this factorial trial was to compare adaptive vs. static goal setting and immediate vs. delayed, non-contingent financial rewards for increasing free-living physical activity (PA).
Methods: A 4-month 2 × 2 factorial randomized controlled trial tested main effects for goal setting (adaptive vs. static goals) and rewards (immediate vs. delayed) and interactions between factors to increase steps/day as measured by a Fitbit Zip. Moderate-to-vigorous PA (MVPA) minutes/day was examined as a secondary outcome.
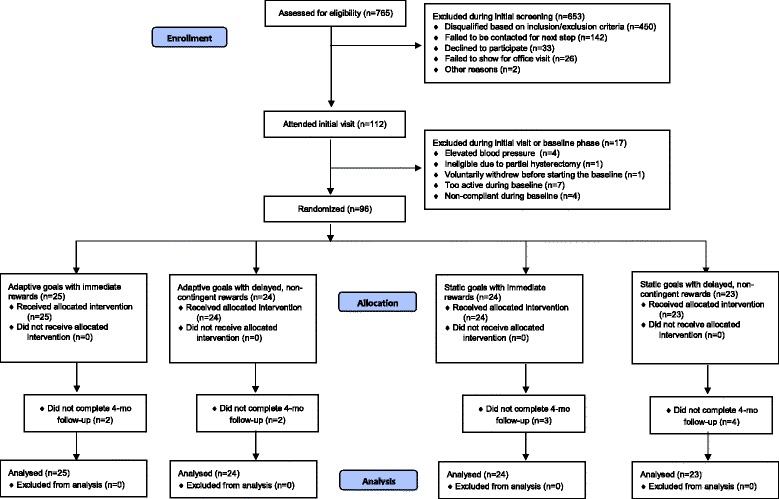
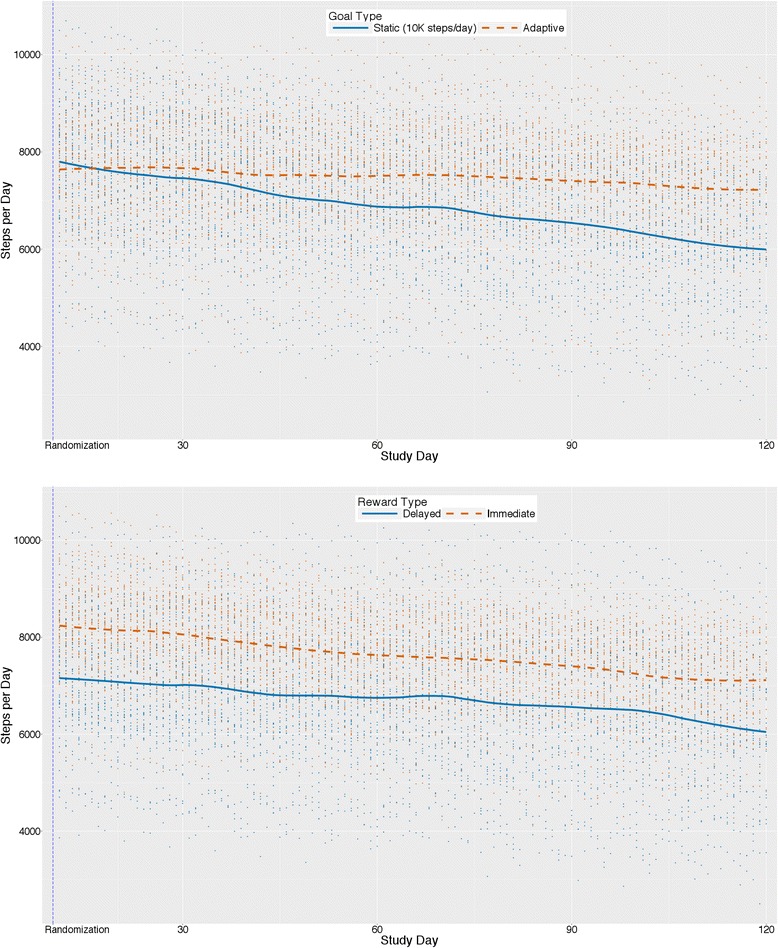
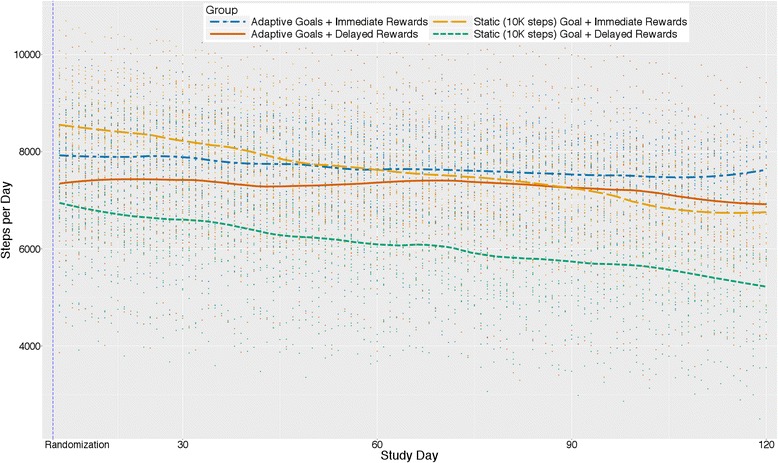
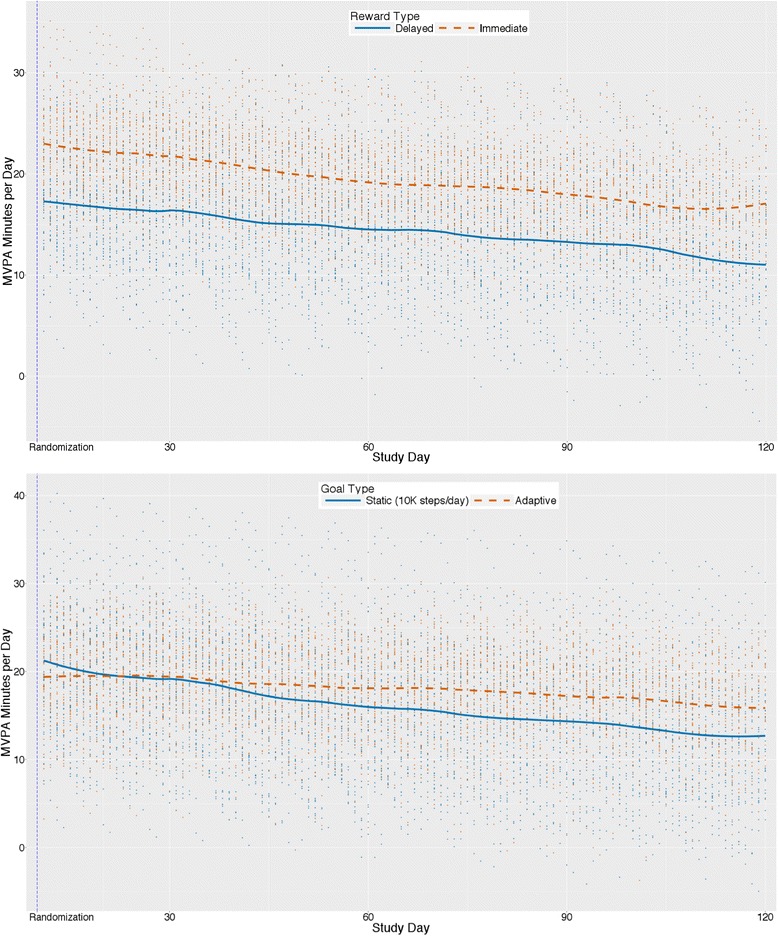
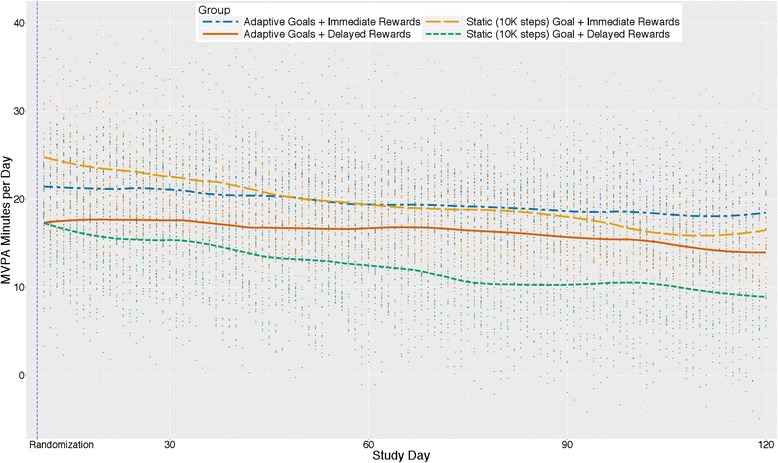
Results: Participants (N = 96) were mainly female (77%), aged 41 ± 9.5 years, and all were insufficiently active and overweight/obese (mean BMI = 34.1 ± 6.2). Participants across all groups increased by 2389 steps/day on average from baseline to intervention phase (p < .001). Participants receiving static goals showed a stronger increase in steps per day from baseline phase to intervention phase (2630 steps/day) than those receiving adaptive goals (2149 steps/day; difference = 482 steps/day, p = .095). Participants receiving immediate rewards showed stronger improvement (2762 step/day increase) from baseline to intervention phase than those receiving delayed rewards (2016 steps/day increase; difference = 746 steps/day, p = .009). However, the adaptive goals group showed a slower decrease in steps/day from the beginning of the intervention phase to the end of the intervention phase (i.e. less than half the rate) compared to the static goals group (-7.7 steps vs. -18.3 steps each day; difference = 10.7 steps/day, p < .001) resulting in better improvements for the adaptive goals group by study end. Rate of change over the intervention phase did not differ between reward groups. Significant goal phase x goal setting x reward interactions were observed.
Conclusions: Adaptive goals outperformed static goals (i.e., 10,000 steps) over a 4-month period. Small immediate rewards outperformed larger, delayed rewards. Adaptive goals with either immediate or delayed rewards should be preferred for promoting PA.
Trial registration: ClinicalTrials.gov ID: NCT02053259 registered prospectively on January 31, 2014.
Keywords: Adaptive interventions; Fitbit; Goals; Pedometer; Reward; Text messaging; mHealth.
Figures
References
-
- U.S. Department of Health and Human Services. 2008 Physical Activity Guidelines for Americans. Washington: U.S. Department of Health and Human Services; 2008.
-
- Centers for Disease Control Prevention Trends in leisure-time physical inactivity by age, sex, and race/ethnicity--United States, 1994-2004. MMWR Morb Mortal Wkly Rep. 2005;54(39):991–994. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
